

Toto's Take: Nature Publication's Long Covid Findings, Incelldx Results, and The Autodidacts of the HealingVrse
Toto's Take: Nature Publication's Long Covid Findings, Incelldx Results, and The Autodidacts of the HealingVrse

Dear Companions,
In short my aunt demanded, that whomever came to see her must at one and the same time, approve of her way of life, commiserate with her in her sufferings and assure her of ultimate recovery.”
-Proust
I found myself gagging on the headline (again)—Biden announces the end of the pandemic. He cut nearly all benefits across the board, from testing coverage to emergency hospital funds. In the meantime, the most senior member of my family caught COVID this week (I wrote this post beforehand). We are not allowed to see her and our family is struggling. So screw you, Biden and ye’ political leaders, and the giant “meteorological” balloon you all rode in on.
Yes the matter of the reality—an ongoing pandemic and Long Covid—is messy, but there is, in fact, a matter to reckon with. For some reason, the complexity of the issue is used to dismiss the existence of the issue. This is a quintessential misappropriation of Occam’s razor.

I may have already lost those of you who are not affected anymore by Covid or Long Covid, but please do share the below with anyone who might be impacted.
Right now, I have at least 50 tabs open on Long Covid. There seems to be a lot of research emerging from clinical practices and small studies nationwide. It is interesting to me how the Covid vaccines were unleashed through unusual and accelerated approval processes, and that was deemed acceptable by all but a small minority, but the clinical experiences of patients and smaller sized studies are dismissed outright.
As you can see in the below image, clinicians are moving forward with over a hundred different interventions affecting different parts of the body.


Why? The answer is simple. Politics aside, patients are desperate. There are 65M people who are sick globally from Long Covid. Many cannot return to work full time. A portion are experiencing significant reductions in functioning.
Among people with long COVID, 79% report having limitations to their day-to-day activities and 27% characterize the limitations as significant.
In the US, even the most conservative estimates put the number of those who are substantially disabled by Long Covid at 5M. What does it mean to care about 5M people? Here is some context.
There are 7.6M Jews in the US. If you are Jewish, like me, you care about this group. Bt even if you are not Jewish, like Kanye, you may care.
There are 1M people with Multiple Sclerosis in the US, and we care about their medical advancements, as it disproportionately affects woman (4x), mothers.
There are 1.3M lawyers in the US, they keep this democratic operation humming.
I don’t know what an effective altruist might say, but these are numbers of people worth caring about.
Fortunately, Nature, a top science publication, has published an article entitled Long COVID: major findings, mechanisms and recommendations bringing the conversation into sunlight. Disproving or proving its findings requires the same thing: Funding for validated studies. That’s the only way to break out of this circular logic—that Long Covid is invalidated on the grounds that there are not properly funded studies to validate it.
Below I summarize some of the recent research and the results of my Incelldx blood test, which purports to identify the bio-markers of Long Covid and the ways to treat them.
The Many Theories of Long Covid
The are hundreds of symptoms experienced in Long Covid Sufferers. Over 50% of suffers see symptom aggravation after Post Exertion Malaise (PEM). Cognitive impairments in long COVID are debilitating, and at the extreme, equal to the UK drunk driving limit or 10 years of cognitive aging, and may increase over time. In reproductive systems, menstrual alterations and declined ovarian reserves are observed, as well as impairments to sperm count, semen volume, motility, sperm morphology and sperm concentration. Long Covid also leads to new conditions —cardiovascular, thrombotic and cerebrovascular disease, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), dysautonomia, especially postural orthostatic tachycardia syndrome (POTS). In other words, this isn’t just a respiratory disease.
But what I have learned is missing, and is necessary, is an organizing principle or theory in order for the medical establishment and society at large to accept Long Covid as a real illness.
There is some consensus forming that there is likely to be several different kinds of Long Covid.
“Long COVID is very unlikely to be one thing.”
- Michael , a neuroscience researcher at Harvard in Cambridge, MA, who co-authored a recent review of possible mechanisms behind the syndrome.
In the article, Lots of Long Covid Treatments, but few are proven, as well as the Nature article, the theories which are emerging can be divided into four broad categories:
Hidden Virus Theory- lurking virus in our tissues cold be causing inflammation or ongoing problems. This is the most difficult to prove, because we need to sample human tissue, which is invasive. Some evidence to support this theory is that the anti-viral Paxlovid clears up symptoms that linger for months in certain individuals. Other anti-virals are being tested by a UK trial called STIMULATE-ICP.
Vascular Disease Theory - does not require the presence of live virus, simply that the virus triggers inflammation and clotting in Long Covid patients. We can see long-term changes to the size and stiffness of blood cells with the potential to affect oxygen delivery. Elevated levels of vascular transformation blood biomarkers in long COVID (ANG1 and P-selectin) both had high sensitivity and specificity for predicting long COVID. This explanation makes sense as fatigue could be caused by muscles being deprived of oxygen. Anti clotting drugs alongside antihistamines are being tested. Virologist Dr. Patterson (with whom I spoke to below) is going after inflammation directly to reduce clotting. He believes fragments of the virus that remain attached to immune cells trigger immune signaling that keep endothelial cells activated and blood vessels inflamed.
Immune dysregulation - with or without reactivation of underlying pathogens, including herpesviruses such as Epstein–Barr virus (EBV) and human herpesvirus 6 (HHV-6) among others. Some of this is commonly noted in other post viral syndromes. Viral reactivation affects mitochondria and has big impact on energy/fatigue symptoms.
Gut Disbiosis- the gut biome is massively shifted after Covid, and there are many markers for Long Covid. For example, Lower Faecalibacterium prausnitzii and low levels of butyrate-producing bacteria are strongly correlated with long COVID at 6 months. I took a GI Map Test By Diagnostic Solutions and found exactly that.
Also, these categories overlap and interact, they shift categorization from article to article. For example, anti-histamines are used in the clotting studies, and are also being tested for how they modulate the vagus nerve to put the brakes on inflammation, since removing inflammation may remove the clotting problem.


Furthermore, the end solution might require running different concurrent treatments, as one issue cascades into other. A butterfly flapping its wings in your gut can cause a tornado in your brain.

Problems of Diagnosis
Exacerbating the issue of gaslighting is the fact that Long Covid research studies tend to document only the risk factors for severe acute illness. But Long Covid has a different underlying biology than acute severe cases.
This is why long covid patients come back with all normal tests, because basic tests such as D-dimer, C-reactive protein (CRP) and antinuclear antibody tests and complete blood count are abnormal in severe, acute cases.
Clinicians are often not familiar with post viral syndromes and often misdiagnose them as mental health disorders in patients. On top of that, only 6% of medical schools fully cover post viral illnesses like ME/CFS, which shares many similar features with Long Covid.
ME/CFS is a multi-system neuro-immune illness that occurs after virus, often characterized by an inability to return to normal activities due to pain or other symptoms, and fatigue. Cardinal symptoms such as post exertional malaise are not widely known, and therefore are rarely included in study designs.
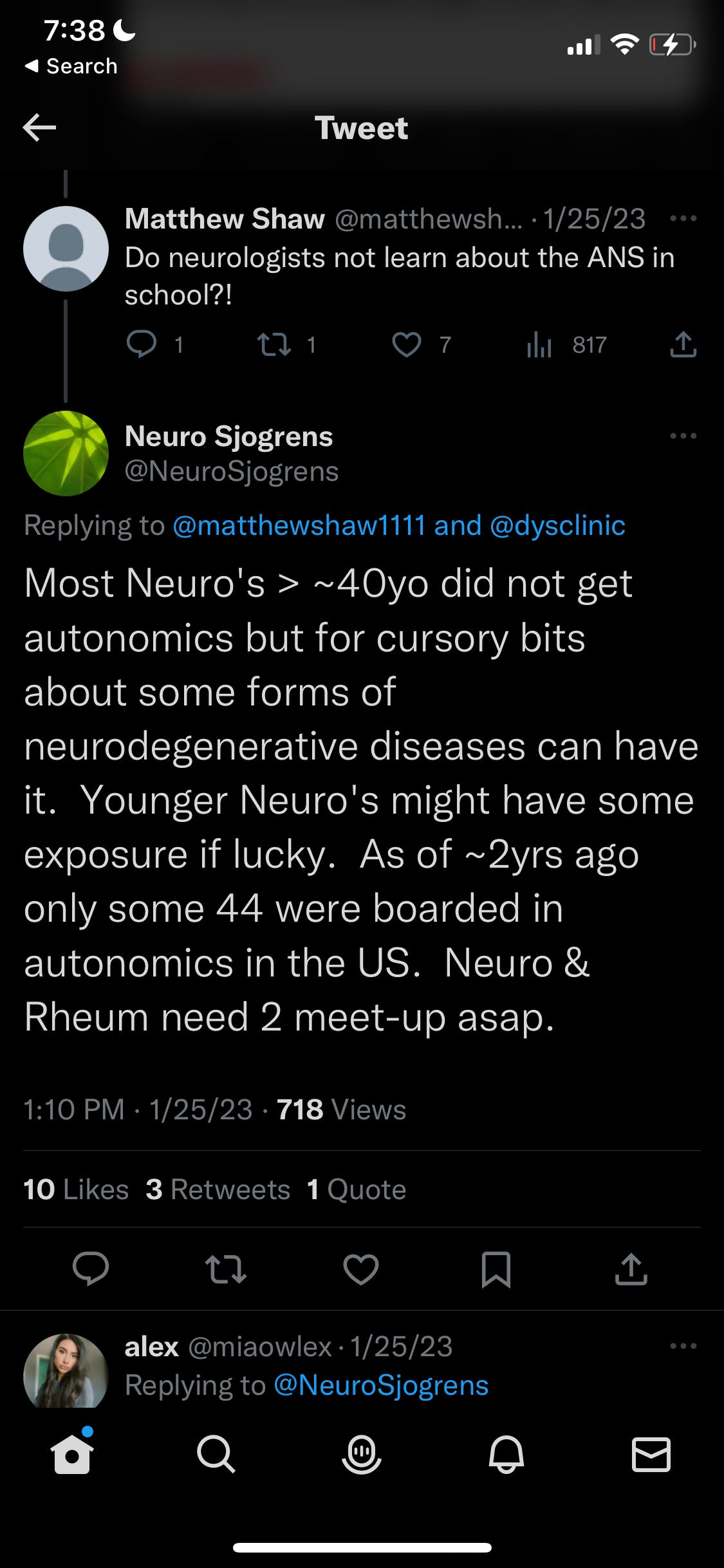
In some cases here, a younger neurologist may actually be a better fit as she may be more educated in autonomic systems. A tweet below highlights why:
Biomarkers
Now there are are many identified different bio-markers coming to light that a patients can test for to see if they are likely experiencing Long Covid.
low cortisol
an array of cytokines
immunoglobulin tests
natural killer cell function tests
the tilt table test
the four point salivary cortisol test
reactivated herpesvirus panels
small fibre neuropathy biopsy
and tests looking for abnormal brain perfusion
Existing Treatments
Borrowing from ME/CFS literature as well as trial and error within patients, here is a collection of treatments currently offered by clinicians:
Instructions on pacing activity, including cognitive pacing (even social media usage can cause a flare in symptoms for some).
Symptom-specific pharmacological options (for example, β-blockers for POTS)
Low-dose naltrexone has become popular for fatigue pain.
H1 and H2 antihistamines, often following protocols for mast cell activation syndrome and particularly involving famotidine, are used to alleviate a wide range of symptoms
BC007, potentially addresses autoimmunity by neutralizing G protein-coupled receptor autoantibody levels
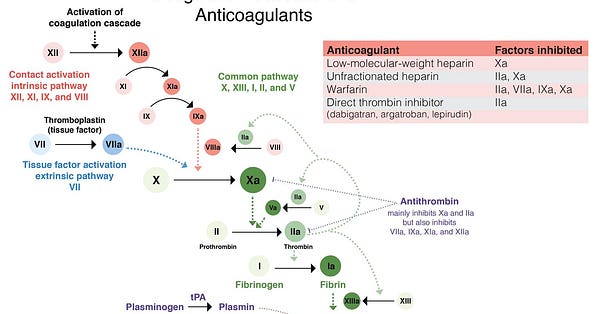
Anticoagulant regimens are a promising way to address abnormal clotting
Apheresis has also shown promise to alleviate long COVID symptoms; it has been theorized to help remove micro-clots and reduce autoantibodies in ME/CFS
Some supplements including coenzyme Q10 and D-ribose.
Other possible treatment options from ME/CFS covering various mechanisms, including improving natural killer cell function, removing autoantibodies, immunosuppressants, antivirals for reactivated herpesviruses, antioxidants, mitochondrial support and mitochondrial energy generation.
My Incelldx test and call with Dr Patterson
Incelldx is headed up by Dr Bruce Patterson, previously an associate professor at Stanford School of Medicine, and virologist who made his name in the HIV field. His team has developed a test, called the IncellKINE test, which claims to identify Long Covid in people with more than 90% accuracy.
Dr Patterson shows up to the 20 minute (sharp!) Zoom call in a white lab coat, which I found to be like a PR move out of the Theranos playbook, and unnecessary. He is forceful and positive. He believes strongly that he has the cure, and that other methods will waste time. In fact, he states: We have the cure for you. It is very enticing to hear this as a person who is looking for a cure.
His 2022 paper explains the science. My totally laymen take: Some monocytes (white blood cells) that patrol blood vessels and are usually discarded quickly (one day or so), stick around in Long Covid, carrying the S1 protein. They are at the heart of Long Covid because they keep the vessels inflamed.
His test looks for a number of cytokines and immune markers, but what is key for each patient to understand is the Long Haul Index. Using machine learning, he has come up with an index which determines the severity of the Long Covid. He says that he has data over 10k+ people who have gone to his site to do the test.
Two months ago I received a score of 4. The highest ratings I found from other people online looks to be somewhere between 10 and 12, so that gave me a sense of where I am in the rating system.
The way they calculate this number is by calculation of certain cytokines, which is a term loosely applied to proteins which are secreted by certain cells of the immune system and have an effect on other cells.
The cytokines IL-2, IL-4, CCL3, IL-6, IL-10 INF-gamma and VEGF were all significantly elevated compared to normal controls. Conversely, GM-CSF and CCL4 were significantly lower than normal controls. Upon further analysis three key cytokines emerged as characteristically indicative of the chronic COVID group (Interferon-gamma, IL-2, CCL-4) and formed the basis for the establishment of a "long-hauler score".
The equation of the LHI index is:
IL-2 + IFN-g / CCL4
My problem was in the denominator, a low CCL4 value. CCL4 is a cytokine which acts like the gas that picks up the monocytes and facilitates their clearance, in this case containing spike. Monocytes that do not get cleared stick around and gain the ability to stick to your blood vessels using something called fractalkine and thereby damage them. This means less oxygen and nutrients are getting to your muscles.
In the numerator, IFN-g is a cytokine that produces the fractalkine causing the sticking, and IL-2 is a cytokine that affects the development of the immune response, specifically the proliferation and activation of T cells, B cells and NK cells. These results were normal for me.
But due to the low CCL4, these monocytes that did not get cleared becoming intermediate monocytes and move around the body using the CCL5 cytokine (which the Patterson test also tests for) as the bus to get around. Using this transportation, they can can go anywhere, even past the blood brain barrier with the S1 Protein. This is why the Patterson team recommends people do not exercise with symptoms as it can cause the spread of these vampire monocytes to other parts of the body. Of course this is contrary to what most medical practitioners have advised to patients who are bed bound or less physically active. And this is why getting to the heart of the matter is important.
One thing I was confused about is that my test results also showed that the S1 was not retained in my monocytes, although Dr Patterson said that if I had tested earlier I probably would have found them. I did show that I had a high number of intermediate monocytes, so indeed they were not getting cleared. I was trying to understand if simply the existence of excessive intermediate monocytes sticking to my vessels can cause damage. I reached out to him on Twitter as well as the smart kids on Reddit for answer but I am still waiting for any reply from the Healingvrse. I will update once I get it.
Clearly a disclaimer on all of this is, I’m just figuring this out as we speak!
Dr. Patterson’s treatment protocol involves Maraviroc an HIV medication which blocks the CCL5 receptors to suppress the monocytes’ ability to travel, and Statins, which lower fractalkine. Without it, the monocytes can’t stick to and damage your blood vessels.
While a newer paper with results of treatment is imminent (I was expecting it would be out already because he had eluded to one on our call), right now it means, you have to decide for yourself if you want to pursue his recommendation—based on a 20 minute zoom call, reddit subgroups analysis of test results, as well as your honorary medical certification as an autodidact (a self taught) person in the Healingvrse.
For us folk, the key is to just understand enough to be able to decide if we want to act on a certain piece of information, since we know we won’t understand it all. The only time I get to talk to Dr Patterson again is if I go on the protocol, in which case there is a 4 week check up with him.
I will be taking next week for family and appointments, so I’ll see you back here on February 19.
With much love from the Healingvrse,
Rebecca
I am sorry about Esther. Checking with your parents regularly. Thinking about you always.
Great insights here as usual, the 5M number is shocking given the lack of media attention surrounding the issue. Would you want to write a post on my substack about your experience? I'm not quite sure how the cross post feature works but would be happy to have you guest post