


trauma, hysteria, & psychogenic illness
trauma, hysteria, & psychogenic illness
chapter II

if you didn’t read chapter one of this story yet, you can find it here:
“trauma, hysteria, and psychogenic illness” cont.:
In the late spring of 2020, at the age of 20, I went to rehab once again. This time, in Chicago. At this point in time I was prescribed Klonopin for anxiety. I took it as instructed, due to my mother only giving me a pill in the morning, and another in the evening; I never had access to the bottle myself. I wasn’t drinking anymore, only smoking weed. Basically I was as sober as I had been in many years. But I was cutting and cutting and cutting. Constantly in the psych ward. My birthday? Spent in the psych ward. Thanksgiving? Psych ward. Christmas? Psych ward. The last stitches often didn’t fall out by the time new ones were sown in.
It was getting more dangerous by the week. Cutting was an addiction for me; I couldn’t seem to stop and yet was desperate to. And everyone I loved was at their wits end. So I got into this dual-diagnosis rehab for women in Chicago, supposedly one of the few that actually treat many clients with exclusively mental health issues. It had three “Cabins”, one specializing specifically in eating disorders, another in mental health, and the third in addiction. I was told I would be a part of the mental health cabin, since my primary aim was to stop cutting. But when I arrived they informed me that actually, anyone who has ever struggled with addiction will be in the addiction cabin. They assured me they address all three issues in all three cabins. This frustrated me very briefly, but I resolved to simply apply every addiction related group to the addiction of self-harm.
They decided to take me off of the Klonopin, since it's an addictive drug I had abused in the past. I tapered off of it over the course of a week or two. Things seemed to be going pretty well here; I had friends, and the groups were worlds better than at the Florida rehab—providing genuine trauma and mental health education. Also this rehab had Behavioral Health Specialists (people who carry out the roles techs usually do, but with education on mental illness, addiction, trauma, etc, who actually help you during breakdowns and guide you through exercising healthier coping techniques. This was immensely helpful since learning how to handle these states of heightened emotions and actually applying these lessons in the heat of such an event are completely different things.) I was still having that bipolar-type cycling, loopy states, and often attempting to self harm, but “it's a process”.
Then one day during a group I fell quite suddenly unconscious. I woke up on the ground only a few moments later. The nurses rushed in to check my vitals and blood sugar; everything looked fine. The nurses were perplexed but thought maybe it was a panic attack. The next day, it happened again. The day after that, it happened twice. Within a week I was purple and bruised all over—collapsing several times a day.
So then: hospitals, hospitals. Getting sent out in an ambulance per concussion protocol every time someone witnessed me hitting my head during a fall. Then visits to a neurologist. EEGs (the primary test for discerning electrical problems in the brain—aka epileptic seizures). Ambulatory EEGs (the kind you wear for forty-eight hours while going about your normal day). MRI’s and tests for blood pressure and heart issues. Another three days in a hospital receiving a heart work up. They found nothing. After weeks of this, at this point collapsing sometimes 20 times in a day, they diagnosed me with psychogenic seizures. Meaning, nothing was physically wrong with me, but my body was falling unconscious due to some unknown psychological trigger.
Then I started having flashbacks—about a week after the fainting began.
So to give some context I’ll mention that about a month before going to rehab in Chicago, I was involved in a violent, traumatic event. They attributed the sudden onset of these spells of unconsciousness to this, saying the delay in its appearance after the traumatic event was probably due to Klonopin dampening my fear response in the month leading up to rehab. Once off the Klonopin, my fear response activated and I started falling out. They recommended continued therapy when I left, the primary treatment for psychosomatic (psychologically engendered bodily symptoms) seizures.
I was at this rehab for 90 days, with the average stay of a client being 3 weeks. But they couldn’t seem to get me “stable”. So towards the end of my time there, they started me on an utterly massive dose of Seroquel, and a normal dose of Lithium. For anyone who knows anything about Seroquel, I was started on 200mg in the morning, followed by 500mg extended release in the evenings. When it hit I was too sedated to walk. My best friend at this rehab, Taya, carried me over her shoulder like a firefighter to cigarette breaks. I laid on the patio and she held the cigarettes to my lips. It's a miserable drug. I slurred my words, slept for days, brain stuffed with cotton.
But my impulsive, raging moods stopped. I wasn't trying to kick the windows out of the group room anymore, fiending for glass (turns out they were plexiglass anyways🙄). I wasn't cutting myself with plastic sheets I sharpened on rocks. I chilled the fuck out.
And I was so desperate to stop with this cutting shit. No one should have to love someone who is doing this to themselves, and people in my life had begun to step away. Distancing themselves from me. They didn't want to be too close when the final blow hit, and I was found dead somewhere. This, of course, is completely rational, and healthy boundaries on their parts. I understood my friends were doing the best they could to keep themselves safe while still loving me from a distance. What I had been doing to everyone was brutal, ruthless, terrifying. So this mixture of mood stabilizers stopped me. And that was worth it.
I was on both Seroquel and lithium for a little over a year. Lithium I tolerated well. Seroquel reduced my cognition to a level of advanced dementia (a very abnormal reaction.) After a few months on this massive dose of Seroquel, I stopped thinking. My brain went quiet. And if a person can’t think, how will they notice they aren’t thinking? My mother became my full time caretaker. I couldn’t finish a sentence without breaking off and asking, “Wait, what are we talking about?”
Conversation was like a game where I spoke the moment I could, hoping whatever I said would make sense in response to what the last person said, because as soon as the phrase was out of my mouth, I would not remember it or the topic of conversation. I couldn’t remember what I did the day before, the month before, five minutes before. I couldn’t remember how life felt before I started only existing for a few seconds at a time. I couldn’t remember if this was normal, couldn’t remember how thinking and memory used to feel. I was a frog boiled slow.
This allegory tells a tale of how to boil a frog. It goes as follows: if you try to dump a live frog into a pot of boiling water, it burns them and they jump out. But if you put them in a pot of cool water, and then very slowly, very gradually, turn the heat up, they will be boiled alive. They don’t notice it's getting hotter. This is what happened to me during the year of Seroquel. I lost a minute amount of cognition, and memory, every day. And after a few months, I no longer could tell if the way I felt was how I had always felt.
I was fainting very rarely now, due to the flatline emotions of a Seroquel life, but started having these indescribable episodes of horror. They were far worse than anything I had ever felt in all those years of suicidality, psych ward stays, and mental illness. I can’t verbalize what these were like, but they changed my concept of mental agony immensely. If they can exist, mental suffering can expand exponentially and indefinitely. I realized all humans are at the mercy of this unfathomable lottery, the stakes of which are worth absolutely no possible reward. There was always an episode of this terrible feeling upon awakening in the morning. My mom had to wake me up with a bottle of orange juice mixed with 8 heaping scoops of red kratom and a packed bowl of weed. I would chug the kratom immediately and rock back and forth, moaning, drooling, unable to form words, panicked, terrified, gripping my blankets desperately until the drug hit twenty minutes later and I began to calm down.
I didn’t understand what these episodes were, and I was having that massive decline in cognition, so I finally started to meet with my first ever psychologist. Before this, I didn’t even ever realize psychologists worked with people on a personal, client level. I vaguely thought they simply studied the mind, in labs and classrooms. Previous to Dr. B, I had only worked with psychiatrists and therapists. In my experience, therapists are there to help you work through your issues: help you process, give you skill sets for coping, etc. Psychiatrists are there to read the DSM and medicate people. Most (though certainly not all) therapists aren’t thoroughly educated on mental illness, medications, or the brain. They are educated on assisting with mental health. They are not usually expert on things like Bipolar, psychosis, Schizophrenia, etc. And psychiatrists, in my experience, never spoke with me for longer than a few minutes.
This psychologist knew so much. He knew so much about the brain, the mind, the psyche. He understood how trauma affects the mind, and he was incredibly versed in mental illness, had worked in psych wards, with psychotic and manic patients. He knew all about psychiatric medicine, about how certain chemicals affect the brain.
Another odd thing about me is how poorly I tolerate psychotropic medications. I get all the very rare side effects. Mostly, they give me neurological issues and movement disorders. I was on 5 medicines at this point just to treat the adverse reactions I got from the Seroquel (making a grand total of 11 psychotropic medications every morning). When I began seeing Dr. B, my mom sat with me during the sessions because I could not finish a sentence without being reminded of what I was saying, and because I would be unable to remember anything he told me.
I had asked my psychiatrist many times if the medicines I was on could be causing my decline in cognition. She replied dismissively, “No I don’t think that could be the cause”. (I had had two long term psychiatrists at this point—excluding the many I’ve seen briefly in psych hospitals and rehabs—, the second was a nurse practitioner at the first’s office. And as I have already said, they always viewed me as an attention seeking, hysterical type. Any issue I have ever raised with them, they clearly doubt the existence of. My psychiatrist had a pattern of nodding sympathetically at my descriptions, telling me some random bit of information I already knew, and then mentioning a new antipsychotic that “might help”.)
I asked Dr. B this same question about the meds fucking with my memory.
“I don’t think I used to be like this. My brain isn’t working. I literally can’t remember anything at all. I can’t think.”
He told me Seroquel works by affecting serotonin, and that serotonin is key in the process of memory. He did not say he had ever seen this happen to anyone before, but he believed me, and explained it's very possible the Seroquel was the culprit.
“Everyone’s brain is different,” he said.
I stopped the Seroquel the next morning. It took about a week and a half for my mental processes to begin returning to baseline functioning. I couldn’t believe my psychiatrists allowed me to live the way I had for the past year. Even writing this now, my jaw clenches with resentment towards those psychiatrists. They did not take me seriously. Due to all the abnormalities of my symptoms, the way I speak about them, and likely the blatant cuts and cigarette burns all over my body, many doctors just do not buy my descriptions of what I am experiencing.
Dr. B was also the first person to teach me how trauma can produce symptoms that can be confused with psychosis. No one, in 5 years of rehabs, psych wards, and doctors, had ever talked to me about trauma and its effects on the brain. I had no idea. It floors me now to try and understand how everyone neglected to address this aspect of mental illness and shocks me even more that my own research did not reach into those realms.
Years after going crazy, trying all sorts of antipsychotics, and entering the period of sedated dementia, heavily medicated for over a year, I stopped all of my meds except Lithium, for mood stabilization, Lyrica, for my “idiopathic pain condition” (another severe and chronic mystery symptom), and propranolol, for a ceaseless and unexplained tremor I had had for three years. So I began experiencing life again without mania and psychosis, and without drugs (well still weed but not really counting that).
Yet I was still hearing and seeing things constantly. Through my sessions with Dr. B, I started to learn about another source of the things people can hear and see.
A flashback is a piece of sensory information that exists within your brain as if it is currently happening. Before this time, I only heard of flashbacks in the sense of a full blown reimmersion into a traumatic event. I thought of them like having some sort of vision—that a person sees, hears, smells, and feels exactly like they did at that moment. As if you are in a fully immersive waking dream. But now I learned that certain sensory details can be stuck, without the full immersion episodes.
In a state of terror, memory is encoded differently. Instead of becoming a part of our greater narrative memory, the sensory information is encoded in the amygdala—the fear center. From there, a trigger can summon the sensory information again, and you experience it as if it's happening right then. This includes any aspect of an experience, including a precise emotional state/inner feeling a person might have felt during the event. So this was the explanation for my “indescribable episodes of horror”. They were flashbacks.
For me particularly, these episodes were initially hard to tie to a source because I lack the ability to visualize things. For example if you were to ask me to imagine a tree, my brain cannot summon any visual image of one. If you ask me to visualize my best friend’s or partner’s face, I see nothing. I can recognize my friends, but I cannot imagine their faces. I have no “mind’s eye”. Ironically, this is also likely a result of trauma. A defense created to avoid unwanted memories.
I am not sure exactly how flashbacks work in people who have the ability to visualize, but mine were hard for me to at first identify because of that lack of visual memory. I heard things and felt things from the past, but both my smelling sense and seeing sense are entirely dissociated from my memories and imagination.
The discovery of the source of those terrible episodes was an invaluable understanding to gain because, if they were flashbacks, I could start trying to recognize what triggers them and avoid those things. For example, I soon realized waking up into streaming sunlight, as I had been doing for the last year, was a major trigger. I got shades for all the windows at the studio and that delivered genuinely life changing relief.
With this better understanding of the way trauma is stored in the brain, I also started writing down the things said by voices I heard. It often sounds like snatches of conversation. Just a few words muttered at a time by one voice. Followed by a couple other seemingly random phrases in another voice. It nearly always sounds as if I am missing the majority of what the voice is saying. Like I am catching two random words of a greater sentence. And the moment after I hear the words, I forget them. So I had never paid the content any mind. They were just random words to me. But as I learned about flashbacks, I started jotting down each word I could catch. And then at the end of five minutes I would have a list of words. And sometimes these lists, when read through like a sentence, were actually a pieces of conversations I knew to be spoken in a past scenario.
This was beyond shocking. I had been hearing this type of stuff for years! And never, ever knew they had any connection to my own experiences. I started writing down the things I heard whenever I could. They often formed into sentences and paragraphs that made sense. And even when they didn’t create a coherent paragraph they nearly always involved very specific themes related to my past.
I couldn’t always be sure they were word for word replays of direct past experiences. But the themes always connected to my experiences. I have very limited memories of my life, so it's possible more of these auditory experiences are direct quotes than I realize. But by nature when a traumatic experience is repressed, it is forgotten and pushed into the subconscious, where it emerges in other forms. For example, think of how dreams work. Often we can wake from dreams knowing immediately what they were in reference to. We can tie them easily to a current stressor or recent event, decoding the metaphorical narrative of dream. But the dream isn’t often simply a replay of “whatever happened yesterday”. The subconscious reworks it into a sort of play-on and reprocessing of whatever is on your mind. A metaphor. So, of course, it's often hard to know what is a direct reference to something I experienced and what is a metaphorical presentation of an internalized idea or memory. But the important point was that now I realized many of the voices I hear in the walls are attributable to this trauma induced sensory stuck-ness. These voices aren’t voices like the kind heard in psychosis.
So now my research was diving deeper into trauma. The classics: “The Body Keeps the Score”, “The Boy Who Was Raised As A Dog”. Others like “Polyvagal Theory in Therapy”.
So there began a new field of personal research regarding trauma’s effect on the body and psyche, and the condition of “hysteria”. Hysteria is the antiquated term for the condition I was diagnosed with a year prior to meeting Dr. B. Nowadays they call it things like pseudo-seizures, psychosomatic seizures, and conversion disorder. In my case, I had the episodes of unconsciousness.
As I came off the Seroquel, the return of my memory brought with it a flood of new memories. Before this experience I didn’t fully grasp the concept of repressed memories. But I began to remember things I didn’t know—and was shocked to realized—I’d forgotten. These new memories triggered months of this hysterical state. (I prefer to call it hysteria because the new terms don’t address many of the symptoms involved in the old hysteria diagnosis, and because—despite the change in derogatory language—I am very much treated as hysterical by most doctors.)
Within these months of acute hysteria, I started to have episodes of paralysis.
Now this was really terrifying. Talk about claustrophobia (when I say I am claustrophobic I’m referring to having severe terror around being trapped or prevented from escaping, not the technical definition of fear of small spaces).
Sometimes the episodes of paralysis lasted hours. The fainting (again I call it fainting because to any observer it looks like I’ve fainted, but if you have ever fainted it feels nothing like that. I would say my episodes are much less uncomfortable than actually fainting. There is no tunnel or black dots in your vision; my episodes are just a sudden collapse into unconsciousness) was of course concerning. But being that I am entirely unconscious during those episodes, it is really mostly scary for those around me.
During the paralysis, I was fully conscious. Eyes open and staring around in panic, unable to move even a finger, immobilized and limp for hours at a time. I worried about having developed a neurological condition, but my primary care doctor “doubted it”, due to the presence of psychosomatic seizures in the past, and he ordered no tests whatsoever. My psychiatrist mimicked this position.
One evening, I was sitting on the edge of my mothers bed, when an episode of paralysis hit. My head fell forward and I slumped off the bed, a heap on the floor, my wide eyes staring into the carpet fibers. My mom was shaking me, trying to sit me up, but I was still unable to move or even talk. After 30 horrible, long minutes, the paralysis ended. My mom was very concerned and wanted me to go to the ER. She drove me to the entrance but couldn’t go inside with me due to it being during Covid and hospitals not allowing any non-patients to enter. She dropped me off and said to call when I was ready to be picked up. I met with a doctor and tried to describe what had been happening to me. I was scared and panicked and my throat ached with the effort of holding back tears. As I spoke with him my legs began violently spasming. They were seizing and shaking so intensely I started to slide off the little bed.
The doctor raised his eyebrows incredulously and nodded as if he understood “what's going on here”, proceeding to walk out the door as I fell spasming onto the floor. I got up once my legs stopped their seizing-shakes and laid back on the little cot, sobbing quietly to myself. An hour later, a nurse came by with a shot of “something that should help.” She dabbed my shoulder with an alcohol wipe, and then injected the medicine. I asked what drug they had just given me and she said, “Haldol and Thorazine”.
This is booty juice! The drug given to psychotic or violent patients to sedate them in psych wards.
I was shocked. They thought I was crazy! (And yes we know I am crazy but this is not an instance of behavioral issues or psychosis). They didn’t believe I could be having a genuine medical issue. They saw it as a behavioral problem, a form of “acting out”, and successfully subdued me. I was quickly too sedated to lift my head. They put me in a wheelchair, wheeled me outside to the street and left me there on the sidewalk. My head was hanging backwards off the back of the chair, and I was staring upside down at the cars speeding down the road mere feet from my limp body. I was too sedated to lift an arm or use my hand and fingers to call my mom to come get me. I was crying and the tears were sliding into my eyebrows and hair. They basically treated my paralysis by sedating me to the degree that I was functionally paralyzed again. It was all wildly scary, trapped within my body in claustrophobic horror.
Some time later my mom just came back to the hospital to wait for my call, since it'd been several hours, and found me in that wheelchair on the side of the road. Head still lolling backwards, neck aching with the unnatural backwards arch of my throat. She had to wheel me to the car and pick me up to lay me in the back seat. This was the last time I sought medical treatment for the paralysis.
I also began having wandering spells. These would probably be diagnosed as dissociative fugues. One evening I found myself lying in a puddle in an alleyway. It was the middle of the night, I was barefoot, and apparently had walked 6 miles in a dissociative state I have no recollection of. This was in a period of sobriety. This was not a black out drunk sort of thing. When I came to, I recognized where I was and that I was pretty close to a good friend's house. I walked to their doorstep and knocked. It was maybe 4am. They opened the door tentatively and then welcomed me quickly over the threshold once they saw it was me standing at their doorstep. When I stepped into the light they both gasped.
“There’s blood all over your face, Scout!”
I went to the bathroom to see for myself and then found several over those finger poking tools (lancets: the things that look kind of like tacks used to test for blood sugar) in my sports bra and I think I had been using them to poke tiny holes all over my face. These episodes happened several times over the course of a few weeks. A few were even more frightening than this one but I won’t write about them.
I began to read a lot of the old ideas within psychology. There is an antiquated diagnosis known as Hysterical Psychosis. It differentiates trauma born episodes of what seems like insanity, from the classical chemically born psychosis. It basically involves trauma driving the subconscious to sort of meld into the conscious. It is described as a waking dream-like state. It involves bizarre behavior, dissociation, memory loss, symptoms like fainting, paralysis, muteness, or seizure-like episodes, delusions, and episodes that look like psychosis.
But when studied from a psychoanalytic perspective, all behaviors are connected to past traumas. Seemingly random episodes of bizarre behavior, are reenactments of terrible events. Or types of metaphorical, symbolic representations of them. The term was changed at some point to dissociative psychosis (which I think is a perfect name for the disorder as it is a version of insanity born of dissociation). There is an old paper about this condition that I have read over and over and if this interests you I highly recommend you take a look at it as well (click this link). So in this I found my answer to probably many of my psychotic episodes, and also feel certain my “loopy moods” are a form of this dissociative psychotic-y state.
Again, really recommend this paper.
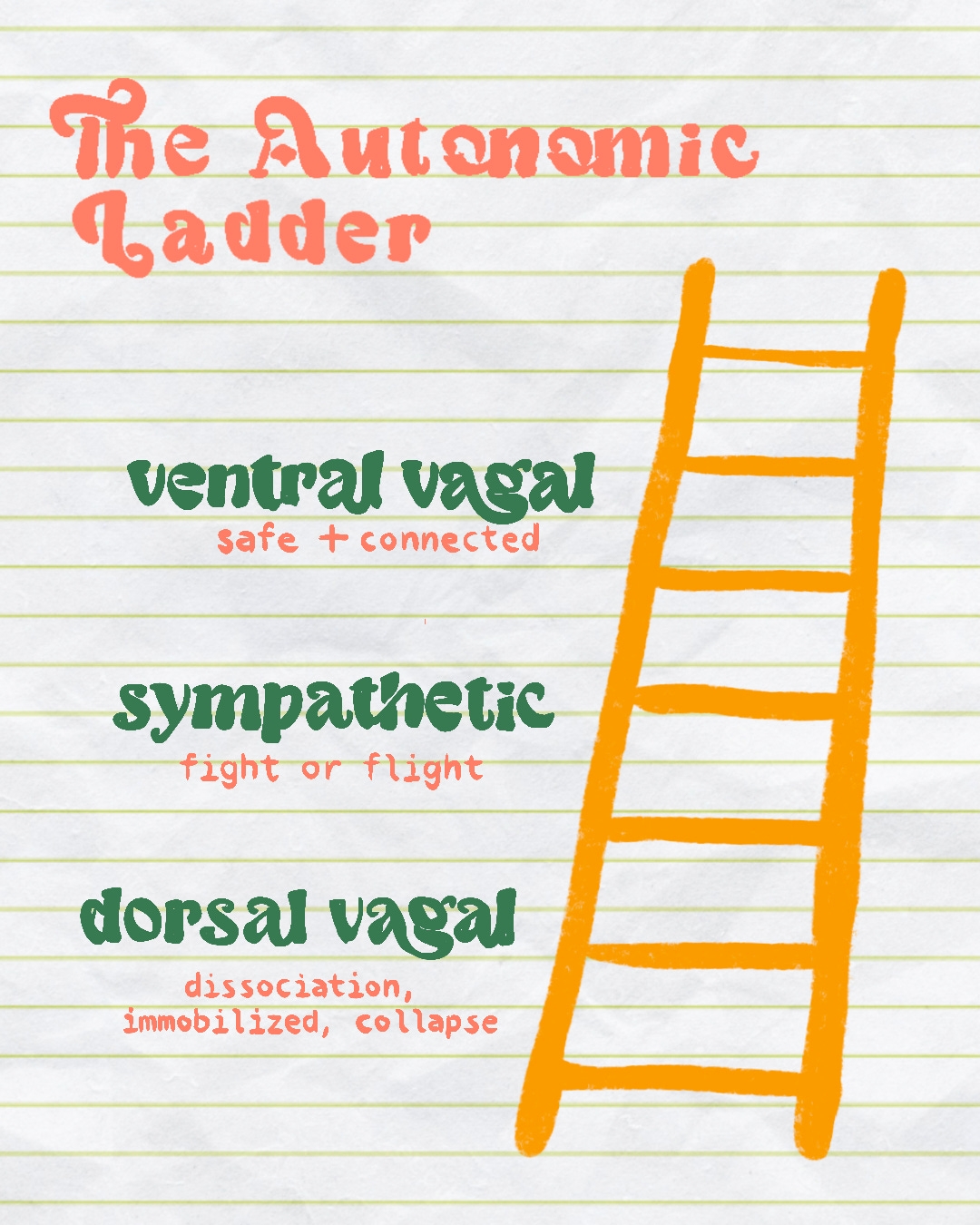
Also, through Dr. B, I learn of something called Polyvagal Theory. Polyvagal theory talks about the sympathetic nervous system and its role in reacting to danger. Within the nervous system there are the sympathetic and parasympathetic systems. Polyvagal theory divides the parasympathetic into two branches, which dictate different reactions to increased fear arousals.

The sympathetic nervous system is responsible for the fight or flight response, also referred to as “mobilization”. Heart rate increases, pupils dilate, your body is flooded with adrenaline, oxygen is sent to the vital organs, and your body reacts in whatever way is needed to regain safety. The parasympathetic nervous system is divided into two branches. The highest branch (furthest up in your spine) is called the Ventral Vagal branch, referred to as “Safety”. It is where ideally everyone should be when feeling safe and secure. It allows for communication, connection with others, feelings of groundedness, presence, and allows your body to perform all the daily functions necessary to retain health. The other half of the parasympathetic nervous system (near the base of the spine) is the Dorsal Vagal branch, also called “Immobilization”. This is responsible for the freeze/faint response and dissociation. It allows for increased pain tolerance, while decreasing blood pressure, accelerating the physical healing process and lowering heart rate.
Evolutionarily, it is theorized the Dorsal Vagal branch is the oldest branch of the system, because at a point in time it was the only possible response to fear. The example often used is of the tortoise. He cannot run, or fight, so he curls up within his shell and waits it out. In mammals, this reaction is enacted in cases of immediate threat to life. An example often used is a gazelle caught by a lion. It appears to “play dead”, hanging limp in the lion’s jaws. And if the predator gives up on it, releases it and moves on, it will slowly recover, give a little shake, and then begin to move again.
The three levels of activation are stacked meaning that to exit the immobilized state (dissociated/freeze), you must briefly pass through the mobilized state (fight or flight), before you can settle at the ventral vagal level of safety and connection. So that little shake the animal gives when they stop “playing dead” is the re-entrance to mobilization as they pass onto safety.
People tend to fall towards one reaction or another when faced with fear. Whether they are more of the “fight or flight” or “freeze or faint” type, is often determined by past experiences of danger. If fight or flight has served them well in the past, this is the pattern they continue to use. If a person's efforts to alleviate fear or distress in the past have failed, and they learn they must “zone out” to get through an experience, they might continue to use this form of defense even when the situation may be better dealt with by a fight or flight response.
In a more blatant example, if someone is in a traumatic scenario, and they are physically immobilized, such as in a bad car wreck where they are trapped in the wreckage, watching the fire burning the car approach them with no way to escape, their bodies can learn to react with dorsal vagal collapse; if someone is in a scenario of helplessness, immobilization, or physical restraint, it can become a pattern their nervous system holds on to.
So this is the explanation for my fainting episodes. (Not the car crash part, I have never been in a bad car crash, that's just an example I stole from The Body Keeps The Score.) But in past states of acute fear and danger, I was prevented from escaping. So my body defaulted to this dissociative response. Something was triggering dorsal vagal collapse in me. People exist within both the sympathetic nervous system (fight or flight level) and dorsal vagal (dissociative) branch and this is very beneficial when it allows someone to zone out certain information and still react to danger. But in my case, it seemed a full dissociative response had been over activated. This created a loss in consciousness in response to a variety of triggers, the majority of which I still have not identified. It is very likely my paralysis is due to this vagal reaction as well. Not causing a complete loss of consciousness, but cutting off my conscious connection to my body, leaving me immobilized. Frozen. Paralyzed.
Many different physical reactions to psychological triggers are a part of this vagal response. People who suffer from panic attacks, for example, get caught in the fight or flight state. Their bodies are experiencing a very physical fear response that is not directly appropriate to a current situation.
Now as I learned more about trauma and the brain, I was understanding that a big chunk of what I had assumed to be bipolar psychosis, (the “loopy moods”, certain delusions, the glimpses, the majority of the voices I hear), are not actually psychosis as thought of in a disease model, but psychotic-adjacent symptoms as a result of trauma. Either as flashbacks, or dissociative psychosis—hysteria.
There is no replacement for the antiquated diagnoses of Hysterical Psychosis or Dissociative Psychosis in the current DSM. Conversion disorder is the closest evolution of that old concept, but it only refers to physical, neurological somatizations of past trauma. It does not refer to the mental and emotional symptoms. And then there are of course PTSD and cPTSD (complex PTSD). These both include symptoms of flashbacks and mood disturbance, but lack any mention of the wild, psychotic-like mix of dissociation and retained sensory fragments.
An alarming number of people are diagnosed with severe mental illnesses, medicated into non-functional oblivion, and never asked about their trauma. Childhood trauma is incredibly pervasive, horribly common. It accounts for a large extent, probably the majority, of mental health disturbances, but as I have said before in other posts, psychiatrists cannot medicate trauma, and the DSM exists in this age almost exclusively for insurance purposes. So, it gets swept under the rug.
I worked with Dr. B for many months, and he taught me a great deal. After stopping the Seroquel I was in a hellscape. Paralysis, ceaseless flashbacks, fainting, and my brain was entirely shut down. I spent every day walking, for hours and hours, the same paths around town. I was very restless, brimming with psychomotor agitation, needing to move and in acute distress, with mental capacities too frozen to find distraction. I couldn’t even turn on a show to watch. I got overwhelmed by the options—I would genuinely would spend hours staring in horror at the overwhelming decision of clicking one of the hundreds of shows on Netflix. My brain was in a constant state of overwhelmed terror, which interferes with decision making abilities to the highest degree. Not to mention I wouldn’t have been able to focus on a show if I even managed to select one.
In my meetings with Dr. B he noticed that I constantly rocked back and forth in my chair and explained to me that the nervous system is regulated by rhythm. I rocked like this all moments spent sitting, standing, or lying for 6 months. Stillness was intolerable. Regulation also accounted for my need to have music playing every waking moment. Why walking was the only thing that offered minute amounts of calm. Step-step-step-step. I was regulating. Regulating the nervous system with rhythm. I also started going to playgrounds and using the swing set for hours every day. I discovered swinging was an especially regulating exercise. I swung until my hands bled and blistered most days. It was the most calming activity I discovered. When I wasn’t walking or swinging I sat rocking back and forth staring at the walls of the studio where I now lived. I was coming to understand myself, but I had never felt worse. In my calmest moments, I was daydreaming of self-immolation and tying nooses when my hands needed tactile distractions.
So, in a desperate effort to make this terrible form of existence stop, I decided to go to a trauma focused rehab center in Santa Fe. I wasn’t using anything but weed and kratom (neither of which I had any plans to stop), but knew I needed to escape my hometown and was aware by this point that some form of trauma processing was the only possible way out of the unbearable state my mind had descended into for the past 6 months. This facility did include the ability to detox clients to a degree, but was mostly a treatment center focused on PTSD and trauma. The groups included trauma education but also a lot of grounding “bottom-up” therapies—therapies basically focused on restoring the body's nervous system.
The term “bottom up” refers to therapies focused on addressing the perceptions within the physical body and restoring it to a feeling of safety, before proceeding to address thought patterns and behaviors— versus “top-down” therapies which first focusing on changing thought processes to influence behaviors in order to calm the body. (CBT and DBT are examples of “top down” therapies). The groups at this rehab involved sound baths, art expression, reiki, massage, equine therapy, EMDR, and gardening, alongside more educational and trauma processing-focused groups. While there I got a better grip on my triggers, processed things to a certain degree and, most importantly, discovered my home town was an incredibly dangerous place for me to exist—mentally intolerable. Within the first day of simply being in another state my mental health improved substantially, even before any of the therapy and treatment.
I also met the sweet love of my life while in treatment there. I left Santa Fe with Franklin in his van, and shortly after moved into that mobile safe haven full time. This is accountable for a massive majority of my first stage of true healing. Having someone I trusted so much, loved deeply, who cared for me, who I felt protected by, and who had dealt with incredibly similar things (specifically Bipolar 1 and severe trauma). We don’t know how we found each other in the midst of this chaotic, painful world. It seems either unbearably lucky, or extraordinarily fated. Our relationship is something that is hard to really convey on paper, but I’ll never stop feeling overwhelming gratitude to God and the universe for allowing me to find him.
I was still having terrible flashback episodes for a while. But having those while safely curled up beneath the pink duvet in the vans fold-down bed with Franklin was a good deal more tolerable than alone in a town of horrors and triggers. My mental health began to improve. I started being able to do small tasks, remembering where I put certain objects when I tidied the van. I began to take a stake in this life I’d found. I felt true joy often. The flashbacks episodes were still unbearable and occurring daily, but in between them I found hiatuses of peace and comfort. My brain continued healing, and the fainting and paralysis were happening less frequently.
The tipping point came when I began taking shrooms. I had used acid many times in the past, but it had been years since I had tripped. Plus, I had never taken psychedelics in such a state of Bipolar mood stability, and never with the security and safety I feel in my life with Franklin. We tripped maybe three times over the course of a couple months, and suddenly I found that my flashbacks were hardly happening at all anymore.
Before this, my ribs felt they would shatter with thankfulness and relief at finding this love and refuge, at the distinctly novel feeling of divine inner stillness I felt when Franklin held me, yet I still lived in daily terror. The indescribable agony of those episodes filled every still moment with a living, breathing fear. A stifled scream in the back of my mind. Knowing they could strike at any moment.
But now, I was coming back to life. I started to occasionally notice beauty in small things. I used to love the way I saw beauty everywhere, magic woven into the universe; I felt my ability to see such beauty amidst the dark and mundane was my special gifting. But for the last couple years, though I looked for it, I could see nothing lovely; everything was tinted with fear.
It's like the way a foreboding musical score can make what could be a neutral nature scene in a movie feel sinister. There was always ominous (metaphorical) music tinting my perception of every moment.
Now I was seeing beauty again, and soon I started to have these tiny daydreams. Simple things. Like planning an outfit for the next day. Wondering what New York city would be like when we got there. Feeling the most gentle eagerness for life blooming inside me. I began to read books and the news. Before shrooms I couldn't think clearly enough, focus on, or remember what I tried to read. And most importantly, I couldn’t care. I could not buy into a plot, lacked all curiosity as to how it would unfold, felt complete apathy towards the characters and storyline.
I continued taking shrooms regularly and the fainting basically stopped altogether. For a while my flashbacks became so rare I hardly thought of them. And then I started to write! I’ve always written but had lacked the ability to exercise this passion in anything beyond my simple journal entries.
Psilocybin apparently has the ability to reconnect parts of the brain that have stopped speaking to one another. And it seems to have done a great deal of re-connecting in my own brain, allowing cognitive functions and emotions that had been blocked off due to trauma to communicate again, and healing the parts of my brain that still lived as if the past traumas were existing currently.
My bipolar seems to be in remission. That year and a half as stable and brain dead as a log, was perhaps what I needed to stop mood cycling. But I also now wonder if I was ever truly Bipolar—in the classic sense at least. I’ve found a lot of evidence in my research surrounding theories of two models of schizophrenia. A disease and hereditary pathway, and then a traumagenic neurodevelopmental model. Meaning one development of schizophenia is due to family history of the disease in certain persons and another course of development of schizophenria can develop purely from trauma, without the classic hereditary pathway. I have yet to find this same dual model introduced in cases of Bipolar. But I wonder about it a lot these days. I feel so sure I was living in bipolar mood ranges for those years. I know what I felt was mania, I know the depression I felt in those days is a different sort than what I feel now. Age 17-20 at least I was experiencing Bipolar cycling. But what if I’m somehow not Bipolar anymore? What if manic-depressive mood cycling can be a product of trauma as well? I have just had to accept that psychology and the brain are still severely beyond our understanding at the moment.
So yeah, the bipolar in me seems to be taking some time off. And much of the severe trauma symptoms, flashbacks, hearing and seeing shit isn’t there, and the fainting and paralysis have all become rarities.
But for the past year, I have been having a variety of odd health problems. Neurological-type-odd health problems.
continue trauma, hysteria, & psychogenic illness here:)