
Excess Mortality is rampant but not for those in charge.
Excess Mortality is rampant but not for those in charge.
Part II: Mechanics. Absence of evidence is not evidence of absence.

In Part I a staggering rise in excess mortality in Canada and across the developed world was discussed. Such sharp increase in mortality was shown to positively correlate with countries that “managed” pandemic the most (through lockdowns and other measures including coerced vaccinations). COVID-19 2021-2022 vaccine administration both in quantities and in the age profile were also shown to be in accord with the biggest contributor to the excess deaths in Canada – Sudden Adult & Infant Death Syndrome (SADS/SIDS). SIDS/SADS deaths were ambiguously unranked and listed in Statistics Canada summary report as “Other ill-defined and unspecified causes of mortality” representing almost half (12,000 out of 30,000) of the total difference in deaths counts between 2019 and 2022 when excluding “Covid deaths”.
This horrible mortality picture cries out for a thorough investigation, in which vaccination must not be hand-waived into irrelevance with infamous “correlation does not mean causation” fallacy. Besides, the mechanisms that have very real potential of turning so obvious correlation into causation do exist in chilling abundance.
Covid-19 Vaccines as a candidate cause
Those who are still under the impression that vaccines in general or the ones for Covid-19 do not cause harm and death, aka adverse side effects (ASE or just AE), should at least accept that this is not the officially held stance on the matter. While the government statistics call ASEs as “following vaccination” or “associated with vaccination”, thus carefully avoiding the implication of causality, there is no denial that at least some of those associations have causal connections.
Looking up “Reported side effects following COVID-19 vaccination in Canada”, for example, makes it very clear that AstraZeneca is associated with thrombosis ASE to much greater extent than the other vaccine vendors, a fact that played into the decision to discontinue its use in Canada. Here’s the exact wording on this from the province of Ontario (emphasis is added):
“Thrombosis with thrombocytopenia syndrome (TTS) is a serious health condition characterized by the presence of acute venous or arterial thrombosis (blood clot) with new onset thrombocytopenia (low levels of platelets), and no known recent exposure to heparin. TTS emerged in 2021 as a new adverse event following immunization with COVID-19 adenoviral vector-based vaccines, including AstraZeneca Vaxzevria/COVISHIELD and Janssen Jcovden COVID-19 vaccines. Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) refers to the clinical syndrome of TTS, in addition to laboratory tests that confirm platelet activation (i.e., anti-platelet 4 antibodies). The province announced a pause on the administration of first doses of the AstraZeneca Vaxzevria COVID-19 vaccine on May 11, 2021, due to an observed increase in reports of TTS/VITT in Ontario.”
Similarly, due to higher rates of myocarditis/pericarditis after Moderna Spikevax among young males, Ontario issued a preferential recommendation of the use of Pfizer-BioNTech Comirnaty COVID-19 vaccine for 12 to 29 years old individuals.
Here is an interesting perspective. More than 20 years of administering the MMR (measles, mumps, and rubella) - a vaccine with not the best safety reputation - registered a whopping 48 adverse side effects of different severity levels. But Pfizer BNT162B2 vaccine beat that fair and square, and, according to Pfizer’s own Cumulative Analyses of post-authorization adverse event reports of PF-07302048 (BNT163B2) received through 28-Feb-2021, registered 1291 adverse side effects (and 1229 deaths) over the first 3 months of the vaccine use. As a side note, the FDA (Food and Drugs Administration) had to be sued under FOIA (Freedom of Information Act) to force the release of that safety report and other documents related to the licensing of the Pfizer-BioNTech Covid-19 vaccine, which would otherwise be kept undisclosed for 75 years.
Some of the most common severe (of special interest) adverse effects associated with vaccines (including COVID-19 ones) are:
Anaphylaxis - a life-threatening allergic reaction caused by hypersensitivity to components such as proteins, preservatives and immune enhancers in vaccines, leading to rapid onset symptoms, including difficulty breathing, swelling, and a drop in blood pressure and in extreme cases, death;
Guillain-Barré Syndrome a serious neurological disorder caused by the vaccine triggering an autoimmune response targeting the peripheral nervous system, which can result in muscle weakness, paralysis, respiratory failure and death; thrombosis – a blood clotting disorders leading to stroke or pulmonary embolism, ultimately resulting in death;
Myocarditis and pericarditis - an inflammation of the heart muscle or the lining around the heart, respectively, particularly associated with mRNA-based COVID-19 vaccines, that cause cardiac dysfunction, heart failure, and death.
So, the ASEs and deaths caused by vaccines are not controversial subjects at all. As a matter of fact, nothing discussed in this essay is controversial or has not been acknowledged by the government health authorities one way or another. The question is not whether the vaccines have adverse side effects and cause deaths but to what extent this is happening and how much of the observed correlation can be legitimately causally connected. And here we enter a very interesting territory!
One may claim that a paper cut or mere appearance of a paper cut can cause death just by arguing that if a subject is already in morbid condition, any however minor stress can become the last straw that broke the camel’s back and thus can be endowed with “The Cause” label. Ridiculous? You don’t say… That was (and still is!) the case with WHO’s guidelines for all participating member states (the world) to attribute death to Covid-19 whenever and wherever the disease could be thought of as a contributor to death (more on that subject in this essay). That is, a previously positive PCR test or a mere suspicion of COVID – even asymptomatic – should be recorded with COVID as the underlying cause of death on the death certificate. By extending the same reasoning to e.g. vaccination, it can be then argued that anyone who dies with a “green vaccine passport” is killed by the vaccine.
An opposite extreme is deflecting causality to something else at all costs. One can claim that a bullet to the head did not cause death, but it was the structural deficiencies of the skull and the lack of the brain resilience to blame. Absurd? You don’t say… That was pretty much the argument to deflect the general claim that vaccines cause autism in the first ever court case won on the matter. The child harmed, Hannah Poling, had a special underlying condition (and nobody knows how many children have the same or similar conditions) that was alleged to had been only “triggered” by the MMR vaccine resulting in autism, so it wasn’t vaccine’s fault, but really the child’s own. But by that very logic, if someone dropped dead from anaphylactic shock within 5 minutes of being jabbed, it would not be the vaccine (which is only a catalyst) but the recipient’s own allergic hypersensitivity that caused the death, would it?
Defining an underlying cause of death is a tricky business. Most mortality statistics show a single cause of death for each individual, regardless of how many conditions that individual had. WHO defines the underlying cause of death for the world as “the condition selected for such single-cause tabulation. In most cases, the underlying cause of death is the same as the starting point. However, sometimes a condition other than the starting point is selected as underlying cause of death for use in the statistics.” So, according to the WHO, besides the actual causality chain, whatever is more useful to be shown in public reports (statistics) could drive the guidelines of how the underlying cause of death is determined. And judging by the aforementioned priority granted to COVID-19 as the cause, it’s probably the WHO that also decides what’s useful and what’s not to be shown in statistics for any given medical or perhaps even political situation.
Considering all those hopeless complications with the “cause”, let’s just explore the so far well-known mechanisms of how a modern COVID-19 vaccines can “trigger” an unfortunate sequence of health complications, which, unlike what happened to Hannah, would apply to any regular person with no finicky health conditions. The discussion is mostly concerned with Pfizer and Moderna products, because of their prevalence in Canada and the USA (50-60 and 40-50 percent respectively) and UK (60-70 percent of Pfizer), but is touching (and has already touched) on AstraZeneca which was used in 30-40 percent vaccinations in the UK and in less than 10 percent in Canada and the USA.
Spike
Spike protein is one of the 4 structural proteins of SARS-CoV-2 virus, which acts like a key, unlocking the door for the virus. Spike (or S-protein) binds to so-called ACE2 receptors allowing the virus to enter a cell and replicate. And this initial interaction isn't entirely benign.
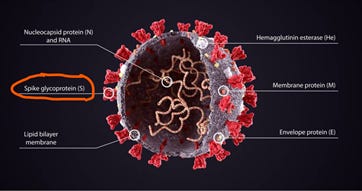
Spike protein in and of itself has deleterious effects by interacting with ACE2 receptors present in not only lung tissues, but also heart, blood vessels and other organs. This leads to inflammation, tissue damage, and dysregulation of physiological processes including damaging endothelial cells, which line blood vessels throughout our body, and causing blood clotting (aka thromboses). The spike protein's toxicity extends beyond direct cellular damage. It can disrupt the delicate balance of the immune system by triggering a runaway inflammatory response, known as a cytokine storm, in worst cases leading to multi-organ failure.
Unfortunately, among 4 alternatives, this infamous protein is the antigen of choice to evoke immune response for both mRNA (Pfizer and Moderna) and adenovector (AstraZeneca) vaccines. Those novel vaccines deliver gene codes that make our cells produce Spike, which is to be as close to any given SARS-CoV-2 variant Spike as possible (ideally identical). Indeed, if it weren’t close to identical, the vaccines would not have been even expected to work.
Within the last couple of years there was an explosion of studies on toxicity of Spike. Many and for sure most of those returned by popular search engines like Google focus on dangers of Spike protein as repercussion of COVID and even use that to encourage vaccination. But those same dangers of Spike apply to vaccines, and unfortunately to much greater extent, because unlike with the virus generally contained within respiratory system, the vaccine-induced Spike protein has a propensity for appearing in great quantities in blood and, consequently, other organs throughout the body.
Cosentino, Marco, and Franca Marino “The spike hypothesis in vaccine-induced adverse effects: questions and answers.” published in October 2022 is an excellent article with a lot of source material that among other things answers a question of “How does production of S protein compare between COVID-19 mRNA vaccines and SARS-CoV-2 infection?”. The gist of the answer is that the mRNA vaccine-induced S protein was found in blood in excessive amounts resulting in vaccine toxicity, whereas the presence of Spike due to COVID infection was detected in similar quantities only through leakage into the blood in subjects who developed severe disease with lung damages. In other words, until one starts coughing out blood and is intubated in ICU, the Spike from COVID does not appear in his blood in any worrisome amounts, whereas with mRNA vaccine it always does.
American Society of Hematology reaffirms that COVID-19 has no special bearing on cardiovascular system when it comes to e.g. thrombosis: “COVID-19–associated coagulopathy should be managed as it would be for any critically ill patient…” And as for the most common mRNA vaccine heart injuries, according to the biggest population-based study on the subject (which, unlike many others, took into account vaccination status), "… post COVID-19 infection was not associated with either myocarditis (aHR 1.08; 95% CI 0.45 to 2.56) or pericarditis (aHR 0.53; 95% CI 0.25 to 1.13). We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection."
It must be said that comparing vaccine adverse effects with COVID complications is one of the many strange anomalous habits adopted into “mainstream” during COVID-19 pandemic. Medications always had high safety standards, driven by "primum non nocere" (first, do not harm) principle, making the whole idea of comparing harm elicited by a pathogen with its medication absurd. So, the author goes with this unsound trend here only because such comparisons are now common even in scientific articles and studies, while maintaining that diseases and their treatments should not be and before were never placed on the same playing field harm-wise, even though in the case of Spike and its potential to trigger harm, vaccine certainly beats COVID.
Another reason for such an unhealthy (no pun) comparison is “long COVID” – a confusing term prematurely coined and eagerly propagated at the time when even the symptoms of this novel ailment were not enumerated, not to mention its likely cause. In today’s scientific literature the “long COVID” is attributed (surprise!) to Spike (so, we might as well start calling it “long Spike”) and the origin of the latter as well as its “long” nature draws attention to mRNA vaccines – and there are reasons for that.

The promise of vaccination (and that includes all vaccines - not just COVID-19 ones) was that the antigen (i.e. Spike) that stimulates our immune system would be mostly localized to the injection site and won’t go around harming other areas of the body. Another pledge was that the key ingredient, mRNA, would be very unstable and would completely disintegrate as soon as it’s done its job. “The cell breaks down and gets rid of the mRNA soon after it is finished using the instructions” promised CDC in November 2020. Well, those promises, along with that Spike protein is harmless, gradually eroded and at this point hold no water at all: Spike protein is definitely toxic, it gets into bloodstream post-vaccination reaching critical organs far away from the injection site, and is found in abundance in blood more than 6 months post injection.
The latter means that the Spike production does not stop and vaccine’s synthetic mRNA is actually significantly more stable than natural messenger RNA upon which the promise of “soon after” destruction was based. Röltgen et al. found mRNA in the COVID-19 vaccines produces spike proteins for at least 60 days. There is research suggesting the possibility that such production of a foreign pathogenic protein could potentially be lifelong or even transgenerational.
There are other harm causing mechanisms attributed to Spike, including those that can lead to immune tolerance and cancer. But let’s just stop right here with a quote from the recent alarming New York Post article: “Beyond cancer, Osborn predicted that a spike would also be detected for other age-related diseases”
How all those mRNA and Spike related characteristics were missed after “more than 50 years of public and private laboratory research” and escaped “the same high standards for safety, effectiveness and quality as all vaccines authorized for use in Canada” remains a mystery, but certainly questions the regulatory processes into scrutiny.
It is important to note again, that this information is all officially confirmed public knowledge. The only arguing is about quantifying the above, and the studies quoted are just examples (might be not even the best ones) and not something cherry picked to advance an otherwise conspiratorial or questionable view. If you don’t like reading dry studies (and who does?), you can go through CDC’s “Understanding mRNA COVID-19 Vaccines” history archive and watch the narrative of the harmless, contained and short-lived vaccine-induced Spike twitching and collapsing. This article does it well too.
But the question still remains how Spike enters the bloodstream? And this seemingly trivial question (don’t we stick a needle in the shoulder, huh?) is actually quite loaded.
Aspiration
Delivering the shot into shoulder deltoid muscle is supposed to and in most cases does avoid veins or arteries which prevents vaccine from entering the bloodstream. But the risk still exists and as we learned earlier, getting mRNA in the blood is no bueno.
Hitting a vein or artery accidentally and thus poisoning the blood was a well-known concern prior to COVID, and a technique called “aspiration” - pulling back on the syringe plunger after needle insertion to see if it returns any blood - was used prior to injecting vaccine.
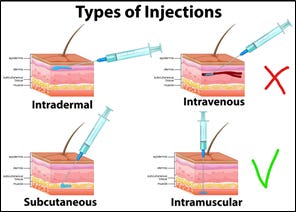
It was standard practice until a few years ago when aspiration became no longer recommended by the WHO. The CDC discouraged aspiration which was parroted by health institutions in other countries, including Canada. Among the assorted mostly administrative reasons given for NOT aspirating, the main one is increased pain since the procedure requires to keep the needle in for extra 5-10 seconds.
“Aspiration before injection of vaccines or toxoids (i.e., pulling back on the syringe plunger after needle insertion but before injection) is not necessary because no large blood vessels are present at the recommended injection sites, and a process that includes aspiration might be more painful for infants” explains CDC in its guidelines for vaccine administration. “Aspiration prior to injection of vaccine is not recommended, as there are no large blood vessels at the recommended immunization sites and not aspirating before injection has been demonstrated to reduce pain.” echoes Canadian Immunization Guide.
The appearance of blood during intramuscular injection into deltoid muscle in adults, however, does not appear to be rare, and that defies the logic of those against aspiration who allege the low calibre of the vessels in the deltoid. A retrospective study reported that 40% of nurses had aspirated blood at least once, and found that “blood aspiration occurred most frequently in the dorsal-gluteal (15%) and deltoid (12%) areas”.
In that context the Alberta’s “Standard for the Administration of Immunizations” (updated in January 2020) sounds odd: “Aspiration is not necessary; however, if blood is noticed in the hub of the syringe, the needle should be withdrawn immediately and the needle and syringe including vaccine contents discarded. A new needle and syringe with vaccine will need to be prepared.”
So, the debate about aspiration goes on, and many countries are less convinced about futility of that procedure. “Based on a precautionary principle, we recommend aspiration before injection.” states Denmark’s Statens Serum Institute in its “Vaccination against COVID-19 - COVID-19 Vaccine Janssen®” guide.
Eureka! The Precautionary Principle! The one that pops up in health institutions as unfrequently nowadays as “first, do not harm”. We don’t need to judge or do exhaustive studies to figure out exactly what percentage of people get vaccines accidentally injected into their bloodstream. It seems that knowing that it does occasionally happen should be enough to promote aspiration. Remember, we are not trying to argue evasive causality – merely the mechanisms.
“We are of the opinion that this cannot be disregarded if one considers that the COVID-19 vaccines will continue to be administrated globally in the form of initial and booster doses. Therefore, the aspiration when giving mRNA and adenoviral vaccines appears to be fully in line with the precautionary principle.” rightfully note two Polish medical scientists in their “To aspirate or not to aspirate? Considerations for the COVID-19 vaccines” paper (emphasis added).
Let’s imagine an unimaginable scenario. You drive through a COVID-19 vaccination station and an expeditiously trained social worker explains to you that if she does not aspirate (which means 10 extra seconds of the needle torture) you stand about one in a million chance (the odds commonly given to being struck by lightning) of developing blood clots in a few months. Will you say “yes” or “no” to aspiration? And how do you feel that that decision was already made for you?
LNP
While injecting vaccine into blood vessels can be considered accidental or rare, there is unfortunately another mechanism which does it consistently and by design – Lipid Nanoparticles (LNP) – a component unique to mRNA vaccines (Pfizer, Moderna) and not present in adenovector ones like AstraZeneca. LNP is a tiny biocompatible enclosure made of lipids – organic compounds, like fat, which repel water and can form structures. Those “fatty” enclosures can be and are being engineered to carry various types of cargo, such as drugs or genetic material, in our case mRNA, to the most remote corners of one’s body.
Here’s a simple description with rich references to various studies on the subject of how mRNA gets ferried around by LNPs: “Intramuscular injection leads to an initial accumulation at the injection site, after which LNPs are rapidly transported to proximal lymph nodes (LNs) by passive draining as well as actively carried by professional antigen-presenting cells and neutrophils. From here, the remaining unprocessed vaccine particles reach systemic circulation [blood] and, depending on the composition of the lipid shell, may be targeted to the liver, spleen or other organs.”
Some LNPs formulations degrade quickly, but ionisable lipids in COVID vaccines have a prolonged lifespan, which, when combined with vaccine’s stable synthetic mRNA, show prolonged Spike protein expression with wide bioavailability in the body.
LNP is a “Trojan Horse” capable of working around our biological defence lines and getting its cargo into otherwise difficult to reach areas like brain or reproductive organs.
For example, the blood brain barrier (BBB) is a highly selective barrier that protects the brain from rogue substances in the bloodstream. As a result, it limits the delivery of drugs to treat brain disorders. And lipid nanoparticles are one of the approaches to overcome BBB and deliver therapeutic agents to the brain for treating neurological conditions like Alzheimer's, Parkinson's disease, and brain tumours.
So, it’s not surprising that this technology was deployed to package, preserve and deliver mRNA into the cells. But that positive aspect of LNP’s being able to smuggle its cargo inside the most forbidden areas unfortunately extends to everything, including where we absolutely don’t want that cargo to be found. According to Pfizer’s own early 2021 bioditribution study (which was corroborated by many independent findings afterword), although the highest amounts went to the spleen and liver, where high cell turnover helps with timely tissue repairs, the LNP, and by implication mRNA, went and was found in all organs, including ovaries, adrenal glands, brain, eyes, heart, testes, uterus, pituitary gland, spinal cord, thymus, bone marrow.
To make things worse, LNPs were also found to carry other stuff that goes above and beyond what claimed to be and was reported to regulatory authorities as useful vaccine ingredients. Ontario, Canada had a special role to play in such a discovery.
DNA litter
Yu et al. were the first to bring up the issue of mRNA vaccines quality and batch variability in October 2021 in an attempt to investigate inconsistent adverse reactions of people (with e.g. anaphylaxis) to different vials, which could only be explained by the presence of ingredients not listed in the official vaccine label and thus not tested for. That raised concerns about mRNA shots conformance to their specifications as well as might explain the wide spectrum of health reactions to the vaccines from different people.
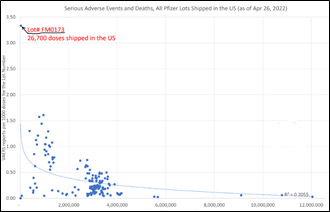
In December 2023, the exact sizes of Pfizer lots shipped in the United States became known via a FOIA data release, including all doses with associated lot numbers shipped as of end of April 2022 to various vaccination centers. The plot below (courtesy of Sasha Latypova) represents the rate of AE’s as reported through VAERS (y-axis) on September 24, 2022 in relation to the aforementioned vaccine batches (x-axis). It shows the staggering inconsistency of the product batch-to-batch. While the seemingly harmless bigger (and thus later) batches are more likely indicative of these doses simply sitting on the shelves, the smaller earlier batches vary from saline-like benign to something as gross as batch FM0173 in the upper left corner which registered a very high rate of 3.3 ASE’s per 1000 doses.
Many independent labs found a variety of peculiar organic and non-organic compounds in COVID vaccines present inconsistently across vaccine manufacturing batches. But among all, DNA molecules deserve special attention as a known trigger for severe adverse effects, cancer in particular.
Speicher et al. reported DNA fragments detected in both monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines obtained from Ontario, Canada. “These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold.” While noting some limitations and the need for further investigation under “forensic conditions” and clarity in “interpreting quantitative guidelines”, the report makes a couple of crucial observations regarding regulatory oversights:
the vaccine production process used for clinical trials and regulatory scrutiny was fundamentally different from the mass production manufacturing, which results in DNA contamination;
DNA contamination regulation limits are dated in light of the novel LNP-enabled mechanism of transporting DNA into cells, without which the otherwise naked DNA fragments would be mostly gobbled up by our immune defences.
“Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs. With several obvious limitations, we urge that our work is replicated under forensic conditions and that guidelines be revised to account for highly efficient DNA transfection and cumulative dosing.”
“Transfection” is what makes those DNA fragments dangerous. A random DNA entering a cell makes that cell produce random protein – and that’s a recipe for cancer. Also, unlike with unstable RNA, the change to the cell function through DNA is permanent from any practical point of view.
Other labs and researchers confirmed DNA fragments in mRNA products. Notably, McKernan et al. found “high levels of DNA contamination in both the monovalent and bivalent vaccines” that were “orders of magnitude higher than the EMA's limit”. That was independently corroborated by Dr. Phillip Buckhaults and his genomics research team. The results of the latter was presented at a South Carolina Senate hearing, and if there is any reference here worth following, that would be it, as in less than 30 minutes you can not only learn a bit about microbiology and lab confirmed dangers of DNA transfection (which even one of the senators claimed to have understood), but also get a practical outlook on how regulatory bodies are set to operate and what drives the academia. (Buckhaults’s presentation at the Senate was taken down by YouTube at least once, so here’s the link where its transcript can be found in case YouTube strikes it down again.)
On December 6, 2023, State Surgeon General Dr. Joseph A. Ladapo sent a letter to the US Food and Drug Administration (FDA) and Center for Disease Control and Prevention (CDC) regarding those disturbing DNA discoveries, particularly in the presence of lipid nanoparticles, and Simian Virus 40 (SV40) promoter/enhancer (we will get to this ingredient next), while appealing to FDA’s own 2007 regulatory guidelines designed to prevent a healthy cell turning into a cancerous one from DNA transfection.
On December 14, 2023, the FDA offered a written response with no evidence that DNA transfection assessments have been conducted to address risks outlined by the FDA itself. And FDA denied the need for collecting evidence because in their opinion the evidence did not present itself from the global mass vaccination campaign (they obviously doubt causation behind tight correlation too).
Ladapo’s reaction to FDA’s response reflects on the precautionary principle we touched upon when belaboring aspiration – just stronger: “DNA integration poses a unique and elevated risk to human health and to the integrity of the human genome, including the risk that DNA integrated into sperm or egg gametes could be passed onto offspring of mRNA COVID-19 vaccine recipients. If the risks of DNA integration have not been assessed for mRNA COVID-19 vaccines, these vaccines are not appropriate for use in human beings.” Also, recently Joseph added: “These vaccines are just products from hell”.
The purpose of offering this Ladapo vs. FDA exchange is not to overwhelm the reader with technicalities, or argue for one side or the other, but merely to point out that FDA does acknowledge both the risk of transfection/integration of rogue DNA into human genome and the presence of DNA contamination in the vaccines. And this, at least in Canada’s case, makes DNA litter a candidate for attributing the “ill-defined or unknown” causes of mortality that drive Canada’s excess deaths through the roof.
SV40
A surprising and alarming discovery was the presence of the Simian virus 40 (SV40) promoter in samples of the Pfizer/BioNTech vaccine, which was notably absent from the Moderna product samples. In October 2023, the regulatory agency Health Canada confirmed the presence of this genetic sequence in mRNA vaccine samples. That was a sensational discovery, which technically should have rendered Pfizer/BioNTech vaccine adulterated.
A fact checker, instead of the intended debunking, validates the finding and confirmation of it by Health Canada. One of the things it gets wrong, however, is the notion that SV40 is used as part of the vaccine manufacturing - hence potential contamination of the final product with its “inactivated” part. SV40 is not used in the production of any of the Pfizer’s Covid vaccines; a study the fact checker cited so frivolously only suggests that SV40 can be used in developing some DNA (not even RNA) vaccines. And that’s what makes it a big deal, regardless of how little or which parts of SV40 were found or where – there is no explanation how this powerful ingredient ended up in the vaccine. Unlike with the DNA chunks originating from the use of DNA plasmids in e-coli bacteria as part of the vaccine manufacturing process, the accidental presence of plasmids with SV40 sequence is impossible, meaning it is intentional and comes without due disclosure.
The presence of SV40 sequence cannot be explained by its known function as enhancer that helps to increase gene expression. As McKernan said, because Pfizer’s vaccines already contain an AmpR promoter, similar to Moderna, the inclusion of the SV40 was “completely redundant” and “all risk, no reward.”
Many other “fact checkers” conflate and confuse the aforementioned DNA plasmids used at the beginning of the vaccine manufacturing process with origins and presence of SV40 DNA sequence. Again, SV40 is not used (in part or in whole) anywhere in Pfizer’s Covid-19 vaccine manufacturing, according to Pfizer. The “fact checkers” also attack a strawman – the presence of the full Simian Virus 40 DNA, which nobody claims. The conflation of DNA plasmid litter and SV40 DNA sequence is often done in the context of “there is no evidence that they cause cancer”. Yes, there is no evidence of that because nobody conducted any studies on humans. And nobody conducted those potentially sadistic studies on humans because in vitro research and in vivo studies on animals showed serious carcinogenic effects of the DNA transfection and effects of SV40 enhancer. So, there is enough evidence to render collecting more evidence on humans at least unethical.
Even FDA engages in strawmanning the SV40 risks, to which Ladapo’s reponse was “… they obfuscated the difference between the SV40 promoter/enhancer and SV40 proteins, two elements that are distinct.”
The presence of the SV40 enhancer-promoter sequence in Pfizer monovalent and bivalent vaccines was first identified by microbiologist Kevin McKernan in April 2023, which followed by a study published in October 2023 and Health Canada confirming the presence of SV40 genetic sequence in mRNA vaccine samples in the same month, which also confirmed the presence of the DNA fragments we discussed earlier, of which SV40 sequence is just an unexpected part. The study’s findings have been replicated by others prompting several international medical organizations to call for the immediate recall of all COVID shots. The presence of SV40 DNA sequences was not disclosed by the manufacturers to regulatory authorities.
To be clear, those studies have not found either full-length SV40 DNA (“monkey virus”), or the cancer-associated SV40 so-called “large T-antigen” sequences, but as Kevin McKernan said “…the presence of SV40 promoters was still concerning due to the risk of them integrating into the human genomes near oncogenes, which are genes that have the potential to cause cancer.”
Dr. Janci Lindsay, the director of toxicology and molecular biology for Toxicology Support Services, concurs with McKernan that the SV40 enhancer could be oncogenic and contribute to causing cancers. She also notes that while the full SV40 virus DNA itself is not in the COVID-19 vaccines, because the SV40 promoter is such a strong promoter, it has high chances of hitting an oncogene and driving cancer-causing gene expressions, or landing on cancerous tumour suppression genes.
It is worth noting that the biggest vaccine advocate, ChatGPT (3.5), whose training data only goes up to January 2022 (at the time of writing), thus making it unaware of the whole SV40 debacle and all the attempts to muffle it down, freaks out at the mere potential for such a discovery, and flatly denies its possibility suggesting that it would otherwise raise significant public safety concern, and cause regulatory scrutiny.

“The presence of SV40 in a vaccine would raise significant safety and regulatory concerns… “
“Any unexpected or unapproved components found in vaccines would undergo thorough investigation and evaluation to ensure they do not pose risks to public health.”
“If a vaccine manufacturer were to include SV40 without disclosing it to regulatory authorities or the public, it would raise questions about transparency and adherence to regulatory guidelines.”
“… the presence of SV40 in a vaccine would likely trigger intense regulatory scrutiny and public concern due to its potential safety implications and the importance of transparency in vaccine development and regulation.”
It did not.
Conclusion
It is difficult to hide a dead body. It begins to stink very quickly. And for the government of Canada as well as other nations in a similar excess mortality predicament the bodies are accumulating into an unmanageable and very smelly pile. The two shelves which Statistics Canada chose to use for such an overflow (and those could be different for other countries), COVID-19 and ill-defined (SADS), are not holding all that dead weight very well and will eventually collapse making things very visible and ugly.
Justification for continued vaccine use based on “there is no evidence that vaccines cause X (cancer, blood clots, myocarditis, etc.)” is indefensible from “primum non nocere” principle alone, and is becoming to look not only absurd but also heinous in the face of all the “coincidental” mortality and absence of any other adequate explanation. Causal mechanisms are there, and statistical data link those mechanisms with the observed effects. The only other type of evidence that can be more conclusive, which is considered to be the gold standard for probing a medication on its side effects, is the double-blinded clinical studies – the studies that either were never conducted properly or the results of which remain unknown.
The presence of SV40 enhancer sequence cannot be explained by accidents and manufacturing quality control issues. So, the only explanation for the presence of this potent undocumented component in Pfizer’s vaccine is that it is there by intent.
In all other cases for all other times, the product (medical or food) would be pulled off the market with recalls, regulatory investigations, and numerous individual and class action suites. Instead, the buyers (government agencies) offered the jab producers full immunity from any harm that the injections might cause and continue to push the “safe and effective” narrative. This reaffirms the intent.
Despite acknowledging the presence of the harmful undisclosed and could not have been unintentional DNA fragments in Pfizer jabs in quantities exceeding regulatory levels, Health Canada stated that they continue to support the use of the COVID injections. “[W]e have concluded that the risk/benefit profile continues to support the use of the Pfizer-BioNTech vaccine”.
How are those shelves holding, Canada, and what’s the intent, eh?