


How to interpret your patients or your own MCG Reports.
How to interpret your patients or your own MCG Reports.
We are automating this as much as possible and as soon as humanly possible

“We have successfully pioneered creating and perfecting a true ‘World’s-First-Ever-Reality-Based,’ proprietary digital signal processing deep machine learning neural network, or an ‘AI’ technology platform. The technology is based on experimentally and empirically proven and clinically beneficial first mathematical principles specifically designed to analyze electrical signals and extract much-needed physiological/functional (mitochondrial networks) biological systems information from animals or humans to aid in making accurate and sophisticated diagnoses that would otherwise be impossible for conventional legacy medical diagnosis tools. These legacy tools include but are not limited to the now 125-year-old OBSOLETE 12-lead ECG combined with telescoping of all the costly, potentially harmful, or even deadly cardiac imaging tests currently used. What MCG detects and measures are far beyond all these legacy tests. MCG functionally detects and quantifies heart or brain (under development) physiological dysfunctions of ANY root causes that have been willfully ignored and neglected in clinical practice; as such, these root causes are missed by the legacy tests, known or unknown to the conventional cardiologists, frankly. Ironically, the lack of focus or curiosity on how chronic diseases arise is the root cause of our legacy medicine’s systematic failures. ”
Building this monstrous system requires ethical, knowledgeable, resilient, determined, and, most of all, morally principled with the best problem-solving creative minds supported by the best computational tools and numerous layers of training datasets to build the digital diagnostic and reporting algorithms to communicate trustworthy vital life-saving messages with the public. Two generations of developers, including mathematicians, data scientists, signal processing and computer engineers, plus one physician, me, yours truly, developed MCG Technology to focus exclusively on saving and extending healthier lives. Building this unique system's deep machine-human-learning process requires time, problem-solving skills, patience, dedication, determination, perseverance, willingness to overcome unimaginable obstacles, and face tremendous personal sacrifices with a decades-long commitment to ensure the delivery of a technology platform that has the safety, reliability, effectiveness, accuracy, and efficiency to expose the root causes of disease, to save lives, vital features which everyone needs. To accomplish this hefty goal, I left my clinical duties in 1998, leaving the plantation behind, throwing everything into one basket, becoming a rebel and a dissident, and embarked upon this epic journey of creation and quest for my freedom!
The datasets range from the electrical signals of humans and animals of various age groups (from the age of 14 up to the age of 100) of racial and ethnic backgrounds as the starting point to other information about their lifestyles, eating habits, food quality/sources, physical activities, or activities, geographic location, environmental & socioeconomic conditions, clinical diagnosis information, medical history, genetic profiles, an equal number of males and females in the data collection process, etc. This information-gathering process is the most laborious, comprehensive, and time-consuming but critically necessary to achieve the goals.
Thus, our work is to apply the best computational engineering techniques to shape and perfect a multilayered natural electrophysiological signal processing system and deep human and machine learning neural network platform to aid diagnosticians in making better and more accurate diagnoses and to monitor the treatment progress and outcomes objectively and quantitatively; our goal is to save lives and extend health span by minimizing or eliminating misdiagnosis, and to stop sending patients to a wrong and dangerous treatment paradigm wittingly or unwittingly causing death and destruction. Competent clinicians can accomplish all these, using our technology platform, at the patient‘s bedside in under ten minutes.
To put things in perspective, language or image processing systems are the other more commonly used AI platforms. For example, ChatGPT for languages, DeepMind for chessboard patterns of human players, Imaging (facial recognition) pattern recognition algorithms, etc., are typical examples. The truth is that with the best technological tools in good people’s hands, good will prevail, but if they are in the hands of evil, human suffering will be the result. Any AI applications designed to appeal to the masses must be carefully watched and reviewed by principled and trusted people, starting from their design phase and continuing ethical approval oversight and control of their development life cycle, version control mechanisms, independent and trustworthy transparent data-collection, vetting, results verification, and validation actions, etc., with an intended goal to ensure consumer protection, safety, and effectiveness. Otherwise, it will be too little and too late.
Thus, I declare: “MCG is the world’s first reality-and -100%-empirical-evidence-based-patient-centric proven, safe, and effective Computational Cybernetic Electrophysiological Systems Deep Learning Technology. The current technology embodiment is a supervised deep human/machine learning platform designed to detect and monitor the earliest signs of trouble and enable primary lifestyle optimization measures to prevent and reverse chronic diseases and extend healthy lives. Perfecting MCG requires dedicated, focused efforts and enormous layers of the most comprehensive datasets possible to aid physicians in timely, safe, and effective diagnosing and monitoring patients’ heart and brain (under development) problems. Especially, MCG can help to make some of the most difficult if not impossible intractable diagnoses using current conventional tools, and decide/assess the treatment choices given to them as safely, accurately, responsibly, and humanly possible.”
Multifunction Cardiogram, also known as the MCG, is the first Artificial Intelligence based computer technology successfully and rigorously validated in real-world clinical settings to revolutionize how physicians diagnose cardiac diseases. MCG is a machined-powered system designed based on systems biology theory, which is the guiding science to discover and quantify the hidden dimensions and features of the inner workings of a biological system mathematically. Integration of all myocardial electrical power required to function under normal and abnormal conditions delivered by sodium (Na+), hydrogen (H+), potassium (K+), calcium (Ca++), magnesium (Mg++) channels and the biological network of 700,000 to 100,000 trillion mitochondria and their mitochondrial ATPase activities of all myocardial cells through multiple cardiac cycles to monitor progressions of ANY disease processes objectively and quantitatively. We need an equally complex system with a massive numerical advantage to warp our arms around: by applying multiple functions expression of the dynamic expressions of the “70,000 to 100,000 trillion mitochondrial biological neuronetwork' ’s power output of the cybernetic principle, the empirically discovered “quinquinquagintillion” numerical complexity, which equals to 1,000,000 trillion parameters, ~10X of the numbers of mitochondria, delivers that required analytical capability. This is the first in the history of humanity.
The totality of the MCG reporting is based on this principle: “Anything, such as Insulin overload (hyperinsulinemia), inflammation (cellular senescence), oxidative stress (tobacco smoking), and anything that suppresses, such as intermittent fasting, fasting, Metformin, etc., the ancient mTOR nutrient-sensing pathway; and conversely, anything that activates or deactivates the AMPK pathway, are fair game for MCG to detect and measure the effects.” We all know that mTOR controls growth to the young and accelerated deaths to the old, and AMPK controls cellular autophagy and more prolonged survival. I decided to link the MCG Platform's outgoing digital biological mitochondrial network power/energy (Dynamic ATP Productions) dynamic productions and distribution patterns as the output to the legacy Med 2.0 disease terminologies/descriptors in my reporting to engender communications and mutual understanding with the establishment types and more importantly for the patients and their caregivers. I translated these terms into the Computational BioCybernetics Systems Electrophysiology Library for posterity.
MCG adopts digital signal processing techniques, multiple mathematical transformations of a pair of digitized resting EKG signals (leads II, V5), then applies empirical clinical data mining, pattern recognition machine learning algorithms to deliver computer-automated highly accurate detection and quantification of ischemic heart disease, along with other cardiovascular pathologies. MCG provides rapid, objective, quantitative, and reliable analysis of a patient’s resting EKG data to assist in diagnosis and to monitor the patients’ progress anywhere with Internet access around the clock. It is designed to address an intractable problem - the lack of an accurate diagnostic tool to diagnose heart disease accurately.
Unlike any other diagnostic system in the world, Premier Heart’s Multifunction Cardiogram allows the clinician on the frontline to make critical management decisions within minutes following data collection and transmission of its highly automated and extremely accurate analysis results without needing an expert over-read.
The FDA has cleared Multifunction Cardiogram in the USA, Japan, and Korea. The MCG test was initially reported by physicians using Current Procedural Terminology (CPT III) Code 0206T. Due to the corrupt practices of the crooked ACC (American College of Cardiology) members of the CPT Panel and their implanted agents in the insurance reimbursement schemes to prevent MCG from taking its rightful position in the markets, most of our end-users bypass the rigged FFS system charge cash for providing the MCG testing/data-analysis-reporting services for an average charge of $350/per test session.
Until now, the diagnosis of cardiac disease, by necessity, has relied almost entirely on costly, inaccurate, and time-consuming stress imaging tests focusing on detecting later-stage, anatomic obstructive coronary artery disease. This, along with all other primary diagnostic modalities, such as nuclear stress testing and invasive coronary angiogram, attempts to identify abnormal blood flow that can be extrapolated to determine obstructive coronary artery disease.
Unfortunately, these tools can only identify large-scale anatomical changes and are not built to detect the more subtle variations and warning signs of potential mortality and morbidity. By merely evaluating large epicardial vessels, one can say that nearly 3/4 of all cardiac vasculature is left undefined and unexplored.
With these conventional methods, small vessel ischemic disease, microvascular cardiac disease (i.e., Syndrome X), metabolic heart disease, and beyond are left to a diagnosis of clinical exclusion. Even more concerning, two large-scale studies1,2 have shown that these tests produce unforgivable false favorable rates of up to 62%! The principal author of the HJM article concluded the following:
Patel MR et al. Low diagnostic yield of elective coronary angiography. N Eng J Med 2010;362:886-95.
Dharmarajan K, Venkatesh AK, et al. Hospital variation in noninvasive cardiac imaging and its association with downstream testing, interventions, and outcomes. JAMA Intern Med 2014; DOI:10.1001. Jama. Intern. med..2013.14407
“In this study, slightly more than one-third of patients without known disease who underwent elective cardiac catheterization had obstructive coronary artery disease. Better strategies for risk stratification are needed to inform decisions and to increase the diagnostic yield of cardiac catheterization in routine clinical practice.“3
The MCG, however, not only avoids this problem but solves it. As an AI-driven computational tool, it replaces the human expert-driven analysis to provide a genuinely objective and, more importantly, accurate report automatically. It evaluates the entire cardiovascular system as a whole and is available 24/7/365.
Over decades of painstaking data-mining of an empirical, clinical database comprised of over 100,000 individuals have allowed the MCG to use digital signal processing to explore the cardiovascular system mathematically. It assesses a patient’s functional variation from a “normal” physiological supply and demand balance, using over One hundred sixty-eight mathematical structural elements from multiple non-linear mathematical functions.
The enormous effort leading to the discovery and implementation of those structural elements provides the vast numerical complexity that enables the exploration of the equally complex cardiovascular system. Before this system existed, detecting pathologies such as myocardial ischemia from resting EKG signals was considered impossible, whether caused by obstructive or non-obstructive coronary artery disease.
The MCG can detect and monitor the electro-mechanical abnormalities analog to myocardial ischemia, whether a large or small vessel, endothelial dysfunction, and other metabolic factors. These include high HbA1c levels due to long-term exposures to glucose toxicity, supply-demand imbalances caused by poor lifestyle choices, the use of drugs, acute blood loss, application of general anesthesia, various environmental toxins, high-altitude sickness, decompression sickness (a.k.a. “the Bends”), the potential effects of weightlessness in exoatmospheric conditions, and beyond.
No longer are we limited to simply describing the degree of anatomical, extensive, epicardial vessel disease. Now, we can pinpoint, analyze, and explain all potential functional causes leading to cardiac ischemia and its effect on the whole cardiac system.
With the MCG, we are capable of the detection, differentiation, quantification, and monitoring of these significant cardiac conditions as a critical tool for primary prevention, along with immediate, intermediate, and long-term outcome measurement in a way that’s fast, simple to use and understand, and objective.
Conclusions from Patel et al. (see note 1 above
Below, you will find a primer for interpreting MCG results. Certain aspects of a test's performance are critical for providing high-quality results, and specific findings need to be holistically and thoughtfully considered.
Once more, the MCG is a sensor/cloud-based computer system that adopts artificial intelligence algorithms culled from digital empirical clinical data and supervised machine learning to create a noninvasive tool for aiding physicians in diagnosing various types of heart disease. However, it does not, on its own, make a final diagnosis of an individual patient.
As stated in the report, when generated, the findings presented in the pathology and physiopathology sections contain comments and suggested diagnoses and conditions, which will require the independent judgment and decision-making of the treating physician who reads and interprets the reports. These should be considered expert opinions and not definitive diagnoses. It is ultimately up to the clinician to make an appropriate diagnosis based on a patient’s clinical history and other relevant factors such as lifestyle, history of substance abuse, etc.
Please note that the last page of the report format contains disclaimers detailing the specifics as had been validated as of 2012.
The assessing of MCG results as a systems analysis allows the clinician to integrate all cardiovascular findings in one cohesive presentation. As with most technology, there may be more than one possible explanation for a specific patient’s results, but considering a patient’s unique circumstances will allow for the most appropriate intervention.
If you have any questions about the testing procedure or the MCG device, please refer to the MCG Start-Up Guide and the tutorial videos on the Premier Heart Website.
The following primer is arranged to follow the format of the MCG report. For ease of navigation, report headings are bolded.
ECG Tracing Quality
Baseline instability can and will significantly affect the accuracy of the patient’s results and, if present, may invalidate all findings, requiring repeated testing.
The tester must confirm that at least four tracings are of marginal quality or better per each test session.
The tracing quality is given such significant emphasis because, due to the mathematics involved in comparing information from the lead II and V5 ECG leads, creating an environment with as little interference as possible within the baseline electrical information is critical.
If you are having difficulties securing a stable baseline for the 82-second tests, the results will not be of adequate quality to be used reliably for evaluation.
A troubleshooting guide for various tracing issues can be found in your unit’s Start-Up Guide.
Ischemia Results / Variability
Severity
Each ischemic score yields information about the state of the cardiac system at the time of that particular tracing.
Intra-session Variability
Variability is not always a consequence of baseline instability and can be caused by physiologic shifts during testing, though tracing quality should always be assured before the testing begins.
While most patients’ scores cluster within a +/- 1 margin, many test subjects will exhibit substantial variation in their scores. This variation reflects shifting physiological conditions and, with variable scores over 3.5, suggests a potentially dangerous situation that should prompt further evaluation to understand what caused such variability, such as a coronary artery spasm or systems dynamic instability.
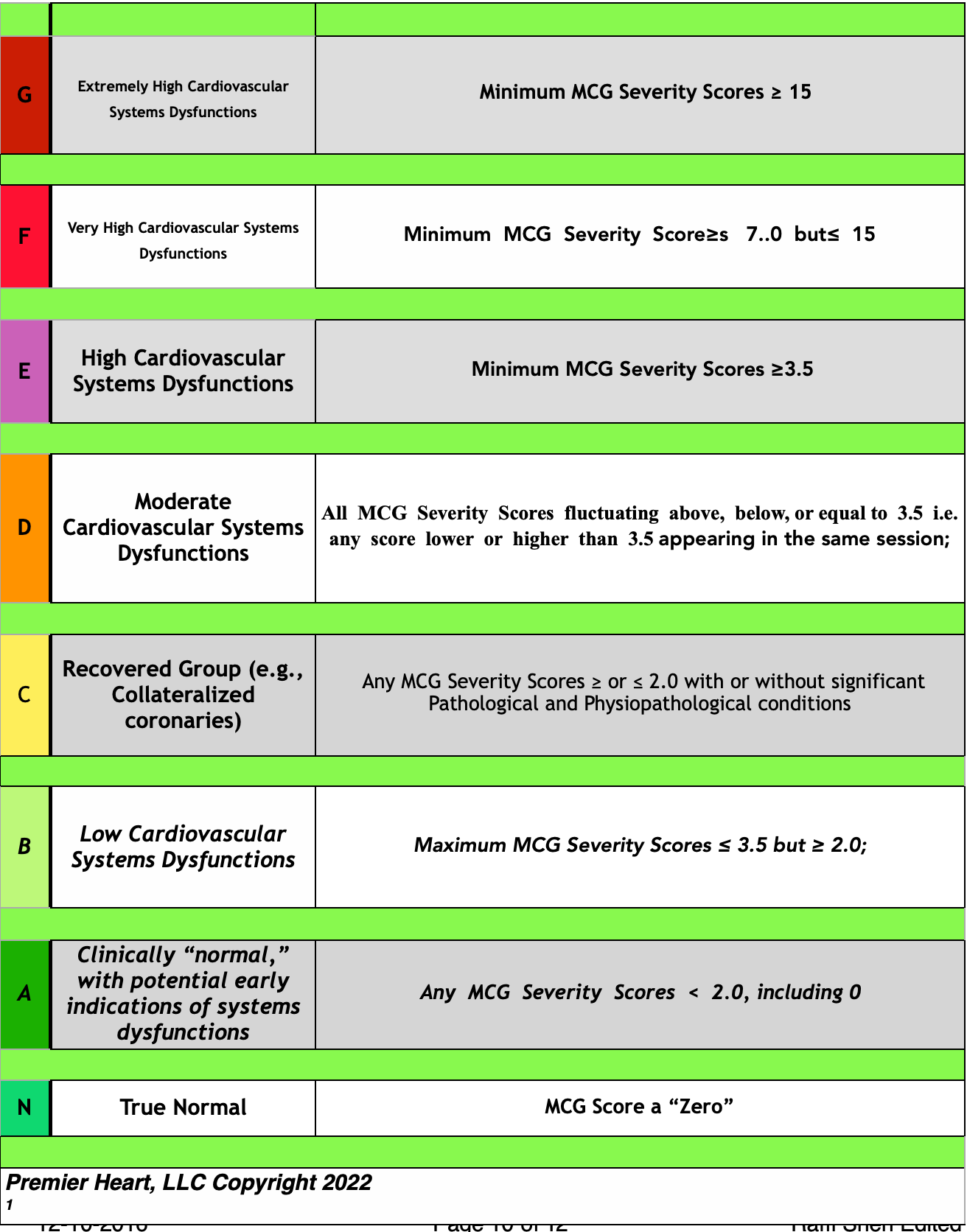
Levels of Severity (please refer to the chart on page 10)
As defined in the specified chart, categories have been extracted from the data to suggest how severe the discovered physiological and pathological patterns are within the patient. The chart itself is designed to assist in stratifying disease severity and management.
The MCG can grade levels of disease severity for the entire cardiac system, including myocardial ischemia (i.e., mitochondrial dysfunction), with lower scores reflecting lower ischemic burden. As the previously specified chart shows, the scores have various implications for management decisions. The categories define how to present myocardial dysfunction. Ultimately, the severity scores should determine how aggressively one must pursue the most effective treatment options, monitor effectiveness using the MCG platform, and follow up for revaluations.
Ischemic Burden Distribution
Global vs. Local
Global ischemia describes one of two conditions:
Intrinsic myocardial dysfunction (i.e., diabetic metabolic dysfunction, microvascular ischemia, etc.)
Significant coronary vascular compromise affecting large vascular territories (i.e., Left Main dx, Proximal LAD stenosis, significant multi-vessel disease, etc.)
Local ischemia is consistent with vascular compromise affecting a regional portion of the myocardium, not the entire system.
Variable categories - global, local, and none
Intra-session variation represents dynamic changes as a result of supply-demand imbalance (i.e., vasospasm, hemodynamic instability)
Global ischemia tells the person interpreting the report that the entirety of the myocardium is involved, which may result from systemic processing involving multiple vessel disease or simply a direct myocardial injury due to systemic cases, such as septic shock. Greater myocardial involvement carries higher severity scores, thus a more significant risk of mortality/morbidity. Meanwhile, local ischemia is frequently associated with single or double-large epicardial vessel disease, reflecting a region of the overall myocardium receiving an inadequate blood supply.
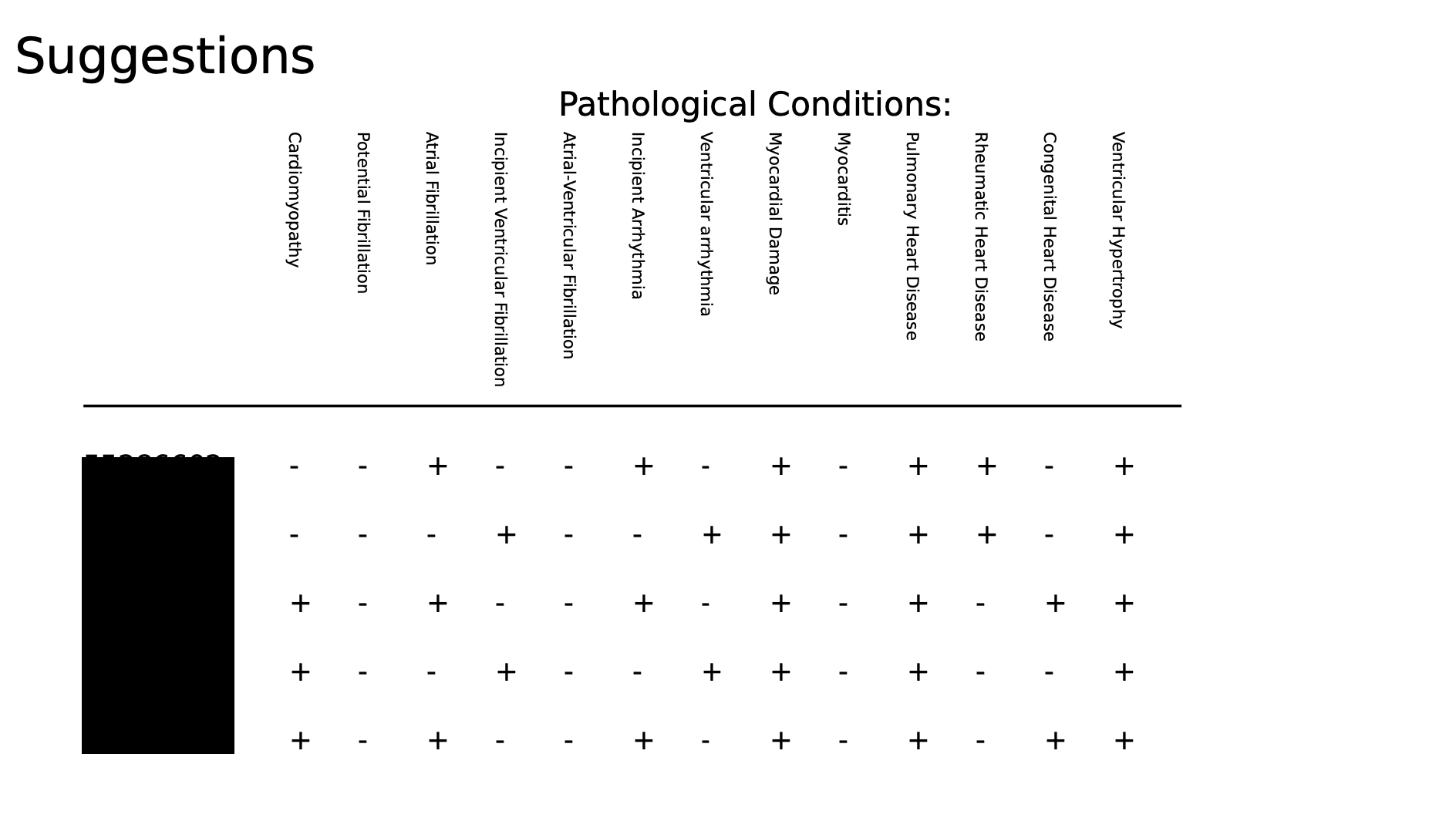
Pathologic Conditions
Pathologic Variations
Myocarditis
Inflammation at a cellular level due to mitochondria dysfunctions due to multiple root causes, including but not limited to metabolic (Hyperinsulinemia) infectious, i.e., parasitical, viral, bacterial, or fungal infections, vaccine-induced abnormal immune response, heavy metal poisoning, highly processed foods, vegetable oils, high Fructose or alcohol intake, excessive visceral fat, chronic exposures to stress, depression/anxiety, illicit drugs, or pharmaceuticals, myocardial injury, post-myocardial contusion, autoimmune disorder, cytokine storms of ANY cause, and environmental toxins, etc.
A primary driver or consequence of all cardiovascular events
The persistence of this variation throughout a session represents an active, inflammatory process. While it may not necessarily be an acute situation, it does describe the potential of an active/sensitive scenario depending on other findings within the report. Examples include systemic infectious causes and recent myocardial infarction. Variable presence implies fluctuating physiology and increasing mortality/morbidity risk but may also be a marker to monitor the resolving inflammation.
Congenital Heart Disease (CHD)
By definition, it is a deviation from the normal that begins at birth.
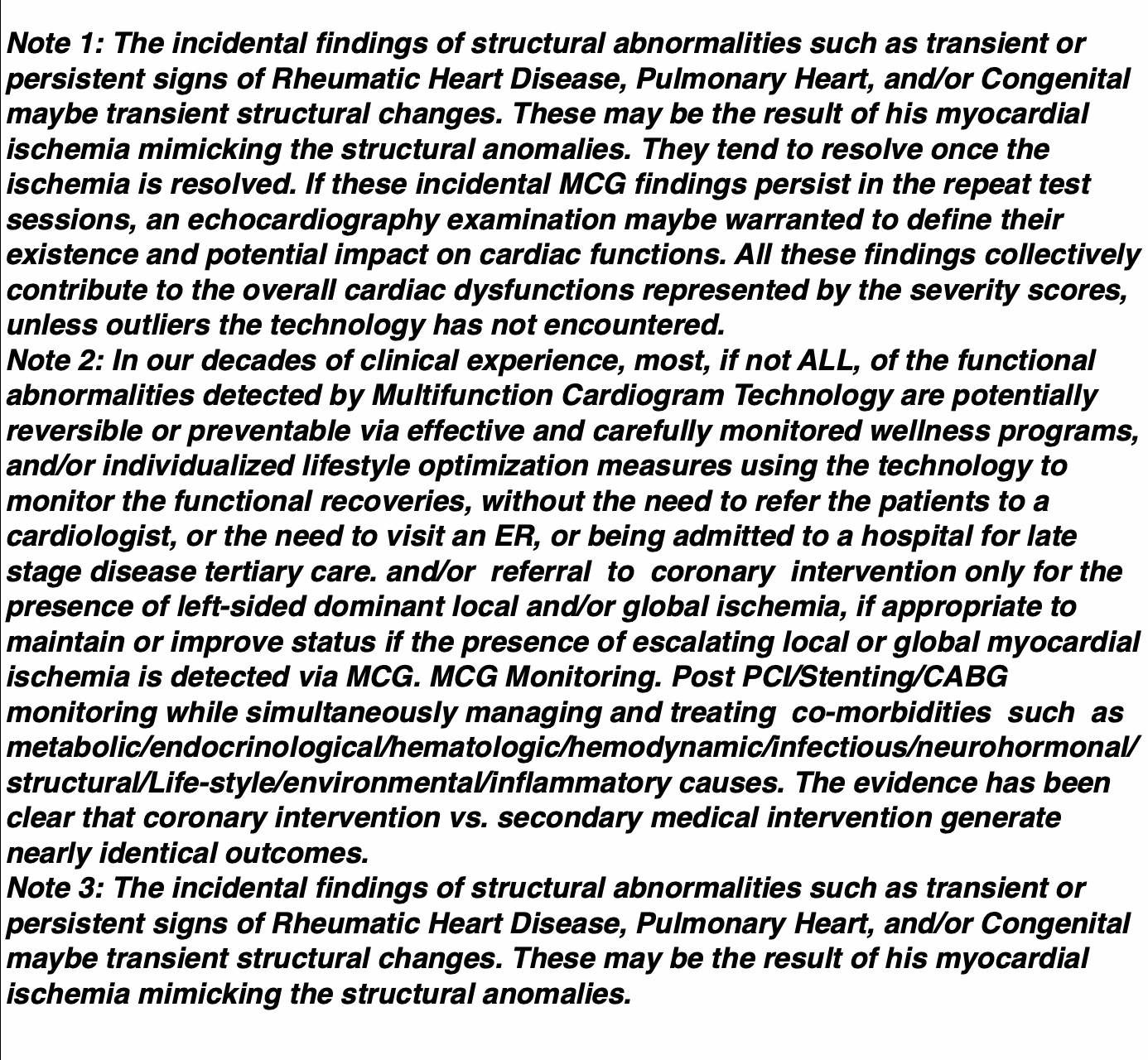
The persistence of this marker during a session suggests congenital structural anomalies. Other functional abnormalities that may result from myocardial ischemia can also mimic CHD.
A longitudinal study may be used to distinguish between these two etiologies.
Cardiac Muscle Function
Cardiomyopathy
Findings consistent with decreased myocardial cellular function
This may be suggestive of early signs of congestive heart failure. Other indications are congenital anomalies,
Cardiomyopathy may be ischemic or non-ischemic. Intrinsic cardiomyo-muscular dysfunction corresponds to significant pathology in a clinical setting. MCG analysis observes subtle variations in the function that can portend future clinical detriment if left unaddressed.
Myocardial Damage
This is the single most sensitive determination of myocardial cellular damage available. However, it is essential to note that its presence is NOT exclusive to myocardial infarction.
A myriad of causes may produce a positive finding. They include:
Myocardial infarct - acute, remote due to coronary artery disease is by far the most common
Hypoxia/hypoxemia
Blunt chest trauma
General anesthesia
High altitude sickness
Decompression sickness (the bends) (7) Infection
Suspicions of acute or recent myocardial infarction should be raised and investigated when myocardial damage, increased myocardial compliance, and Myocarditis persist in the same session.
Ventricular Hypertrophy
Findings consistent with increased cardiac mass, most frequently associated with, but not limited to, hypertension.
Hypertrophy often co-migrates with findings that drive conditions like rhythm disturbances and other pathophysiologic variations, such as myocardial remodeling.
Rhythm Disturbances
All findings are associated with variations from normal sinus rhythm. Reports indicate the presence of arrhythmia, the isolated occurrence of the disturbance, or the prediction of future clinical manifestations.
Potential Fibrillation
Atrial Fibrillation
Incipient Ventricular Fibrillation
Atrial-Ventricular Fibrillation
Incipient Arrhythmia
As with other MCG findings, these can precede clinical presentations, sometimes by years. Care must be taken to utilize the early notifications as expeditiously as possible. In the case of moderate to severe ischemia or other pathologies, these findings could be just under the surface. Further evaluation, especially in the cases of intra-session variation, can be extremely important for the patient’s long-term safety.
In the case of patients with present symptoms, these findings should be more thoroughly evaluated using the MCG Personal Monitor or ECG Event Monitoring.
Valvular Considerations
Findings consistent with variations from normal valvular function
Clinical Correlation with Historical Systemic Infections
Pulmonary Heart Disease
Right heart valve issues
Right heart failure
Systemic infections with a pulmonary focus
Possible pulmonary hypertension
Rheumatic Heart Disease
Left heart valve issues
Systemic infections with full-body involvement
While many of these results relate to intrinsic valvular issues, many will be subclinical for the patient. It is typically caused by the aftermath of a prior history of systemic infections that have left their mark on the cardiovascular system.
The persistence of this marker during a session suggests structural anomalies, but functional abnormalities resulting from ischemic etiology may mimic this pattern. A longitudinal study may be used to distinguish between these two etiologies.
Pathophysiologic Variations
Myocardial Responses
Myocardial Remodeling
Evidence of Myocardial Compensatory Response
Decreased Myocardial Compliance
Increased myocardial stiffness
Increased Myocardial Compliance
Decreased myocardial stiffness
Combined with Myocarditis, it is very suggestive of near-term (~6 weeks) myocardial infarction.
Clinical Myocarditis is a leading cause of increased myocardial compliance
Acute Power Failure (acute mitochondrial function loss)
Power is defined by the cardiac system’s overall power output
Failure when the work falls below a standard threshold
This finding reflects inadequate overall functional performance not limited to left ventricular output
Depending on that condition, a spectrum of acute and chronic clinical conditions may present with acute power failure and can be temporary or permanent.
All of these myocardial variations have relatively straightforward correlations. Myocardial remodeling will coincide with historical or persistent ischemia or injury, requiring a compensatory response. Though, with the case of, say, long-distance running, this remodeling may be
Physiological. There also may be an injury that does not present with remodeling, suggesting that it is either in an earlier stage or has failed to elicit a compensatory response.
Myocardial compliance speaks to the responsiveness of the myocardium to stretch and adapt. In the setting of increased compliance (a previously largely untestable concept), the muscle has a laxity, which has been identified in recently injured tissue. Decreased compliance is a well-understood concept consistent with significant tissue damage and the failure of the myocardium to relax. Typically, this co-migrates with myocardial injury and remodeling and suggests a potential for congestive heart failure. These two measurements can co-exist in some instances at times.
Acute Power Failure can be closely tied to decreased myocardial compliance following damage and remodeling, telling of potential congestive heart failure, along with various other situations and circumstances. Functionally, this is connected to eventual decreased cardiac output.
Rate Variations
Bradycardia
slow heart rate (<60 BPM)
Tachycardia
fast heart rate (>100 BPM)
These categories purely reflect heart rate. Bradycardia is seen regularly in individuals with high vagal tone and would not necessarily be considered abnormal. Tachycardia is a non-specific indication of rapid heart rate and thus could relate to many causes.
Electro-mechanical Synchronization
This is a synchronization measure between leads II and V5 over multiple cardiac cycles in the frequency domain (vs. traditional milliseconds vs. millivolts in the time domain).
Asynchrony described here is different from what has been historically described as Asynchrony. This is not just TEMPORAL synchrony but the degrees of de-variations from regular synchronization between the signal input and the output from leads II and V5 or vice versa.
Global Asynchrony (II < V5)
(2)Global Asynchrony (V5 < II) (3)Localized Asynchrony
Local Asynchrony (II < V5)
Local Asynchrony (V5 < II)
Lead II can be perceived as a right-sided cardiac function, and Lead V5 is oriented to the left ventricle. In the descriptors, the lesser side represents a delay in synchronization compared to the more fantastic side, which can be considered the lagging or pathological side. Like this, II<V5 suggests a right-sided pathology in the Right Coronary Artery, or RCA, dominated myocardium territory. Paradoxically, one can have a wholly occluded left-sided coronary vasculature effectively collateralized by the right-side coronary supply. The active ischemia/supply and demand imbalance leads to right-sided asynchrony/functional delays due to the increased workload to supply both sides of the cardiovascular system. The reverse can also be true,
Global Asynchrony carries greater mortality/morbidity risk. When there is a combined, more likely Global Ischemia or less likely Left-favoring Local Ischemia, Left Ventricular Hypertrophy, Remodeling, and Persistent Tachy-Ventricular arrhythmia linked to the global Asynchrony. However, even it is less likely that due to the left-sided local Asynchrony, the increased myocardial compliance (implying an active acute process), and fluctuating severity scores in a session in ANY category, plus the techy-ventricular arrhythmia, there is a dramatic increase in the probability of near-term sudden cardiac death. Close monitoring to identify the triggering agents is critical to ensure reversal.
Please see the perfect real-life example below:


Even though his first MCG test session was categorized as category “B,” a high “B,” tachyarrhythmia of the ventricle, and right-sided local ischemia, this gentleman was warned of the danger of a hemodynamically unstable heart with increased risks of sudden cardiac death, significantly when the follow-up sessions showed rapidly growing severity scores thus accelerating towards the elevated categorizations over a short time interval; he was advised to be monitored biweekly at the least to start dramatic lifestyle optimization intervention and complete medical therapy optimization to reverse the dangerous, life-threatening conditions he was in. Our advice was ignored, unfortunately. Four months later, he suffered a cardiac arrest and was legally dead for eight minutes. Fortunately, his cardiac pulmonary resuscitation efforts were successful. He woke up from a short eight-minute flatliner. The lesson learned is that MCG bought the precious time that would have allowed his physician to identify the offending trigger and mitigate or eliminate the threat to his life. Also, the initial lower category level (Category B) gave him enough reserve and a greater likelihood of surviving the sudden death episode. He got a second chance in life.
A follow-up test session is scheduled. This report will be chosen as another cautious example for training purposes.
Localized Asynchrony is typical of specific areas of myocardium out of synch, likely secondary to localized hibernating myocardium caused by localized ischemia.
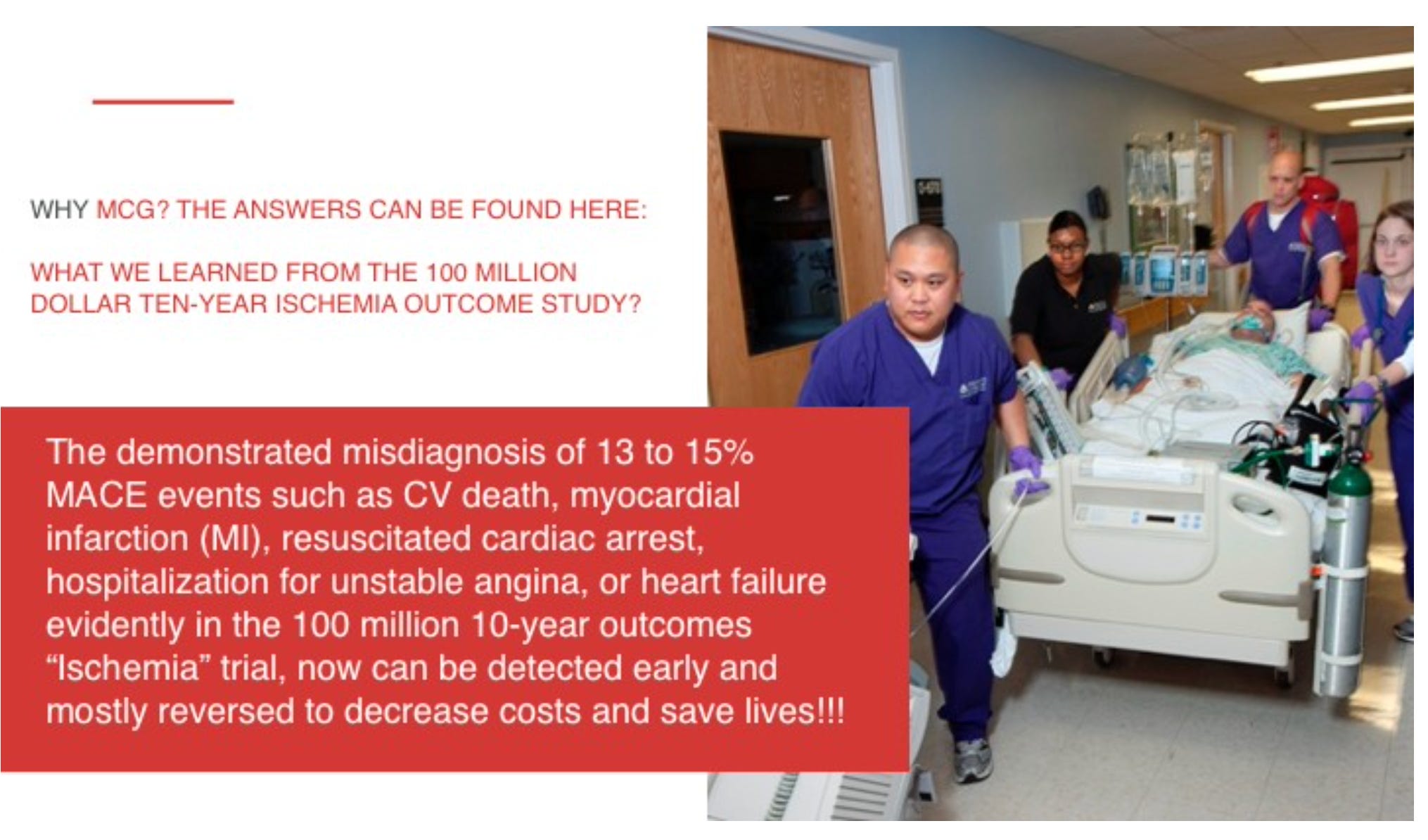
More importantly, the latest long-waited “Ischemia” trial results have finally been revealed: https://www.ischemiatrial.org/ischemia-study-results. The most glaring part of the datasets from both arms of the trial is - that both arms missed 13-15% of the patients who suffered from MACE. MCG will make a considerable difference in identifying these patients early and enable disease reversal if given a chance. No one needs to suffer under the threat of MACE!
LEVELS OF SEVERITY:
Where are these available?