

Why Childhood mRNA Vaccination is So Dangerous
Why Childhood mRNA Vaccination is So Dangerous
Lasting Immune System Damage
July 18,2022
The June 16 edition of Real Health Flash, Clot Shot Recommended for Children, outlined the seriously flawed reasoning behind FDA’s authorization of COVID-19, mRNA vaccines for children as young as 6 months.
We noted at the time the limited duration of the trials prevents us from knowing the long-term consequences of mRNA vaccination on children.

Since then, we have begun to piece together a more complete picture of the effect of mRNA vaccines on young immune systems and conclude children are especially at risk of long-lasting immune damage and subsequent respiratory viral infections.
Before discussing special childhood mRNA vaccine risk, let’s review what is known with a high degree of certainty:
COVID-19 and Children
· Healthy children are at extremely low risk of severe illness from COVID-19
· Around 75% of children in the US are COVID-recovered and have natural immunity
· Natural immunity is robust and long-lasting and superior to the protection from mRNA vaccines
· Previous Omicron infection highly protective against variants – Wuhan COVID-19 vaccines not so much
· Children are not COVID-19 spreaders
· There is no COVID-19 emergency to justify FDA’s issuance of an Emergency Use Authorization (EUA)
· Childhood vaccines granted EUA status based on laboratory measurements of transient rises in antibodies (“immunobridging”) and not clinical effectiveness
· There is no correlation between antibody levels and clinical outcomes
COVID-19 Vaccine Dangers
· The original Wuhan virus was a bat corona virus “enhanced” (gain of function) with a genetically engineered spike or S protein designed to make it more infectious
· The spike or S protein has the highest rate of mutation, rendering vaccines out of date before they are even distributed
· The spike or S protein portion of the Omicron variant is rapidly mutating as could be expected, with BA.5 the most infectious and rapidly spreading variant at this time
COVID-19 Vaccines are Non-Sterilizing
· mRNA vaccines are non-sterilizing, meaning they don’t produce antibodies that kill the virus as do most other vaccines
· Traditional vaccines are based on the whole virus (not just the S protein), that is live but disabled so it can’t replicate (e.g. measles, mumps, polio, etc.)
· Whole virus vaccines produce sterilizing antibodies that kill the virus
· There has never been a successful vaccine (whole or mRNA) for a respiratory virus due to the high frequency of mutation
· Efforts to create a vaccine for SARS-CoV-1 completely failed and killed off the test animals
· The most prominent Omicron variant, BA.5 preferentially infects the vaccinated only 3 months after immunization, in contrast with lasting COVID-19 protection from natural immunity
· The highest rates of infection, hospitalization and death are among the vaccinated
· Adolescents and young men have a much higher incidence of myocarditis or pericarditis following mRNA immunization than those with natural immunity
Now here is the scary part. Children’s immune systems are extremely vulnerable to harm from non-sterilizing mRNA vaccines.
What is different about young compared with mature immune systems: immature systems must spend the first few years learning how to adapt to external threats from viruses, bacteria, fungi, and so forth.
Newborns have maternal antibodies for about the first 6 months of life to help protect them. After that, they need to develop their own immune capability that can respond to infections.
Innate (Rapid Response) versus Adaptive (Memory) Immune System
Infants have all the tools necessary to become fully functional, but it takes time and experience from exposures to real-world threats to mature. These tools include a rapid response system to active infections known as the innate immunity, and a longer-term, memory system known as adaptive immunity.
The innate system mounts an immediate antibody response to a foreign invader in order to help stall an infection while it calls for backup from the adaptive immune system through chemical signals.
Antibody tests recorded during the childhood COVID-19 vaccine trials noted above (immunobridging) refer only to the short-term innate immune system. These bursts of antibody production peak and then go away after a few weeks or months.
And they don’t kill the virus, so are called are non-sterilizing.
Adaptive immunity backs up the innate system’s rapid response to foreign invaders by detecting signals sent by the innate system under attack and marshalling additional resources to join the attack and clean up the aftermath.
Adaptive system has a long memory for threats
The adaptive system also serves as a library of potential threats, storing cells with a memory of previous invaders and rapidly responding with specialized cells to future infections. The adaptive system is also highly flexible with built-in redundancy, responding to countless variations of previous threats.
It is said that the adaptive system can effectively respond to hundreds of thousands of variants of a particular infection by identifying viral components that are less likely to mutate over time.
Vaccine-induced immunity focuses primarily on the spike or S proteins and mutations to this region mitigate a strong immune response to variants, making reinfection more likely.
In contrast, natural immunity will recognize a full complement of protein and other chemical markers on the virus and mount a robust immune response, making reinfection or serious infection less likely.
Learning to differentiate invader from self
An essential part of the learning process of young immune systems is the ability to differentiate foreign invaders from self.
Viruses often cloak themselves with surface proteins and other compounds that resemble host cells so they can hide from the immune system. Many respiratory viruses share a similar cloaking chemical signature.
A child’s immune system needs to learn that when the system is activated it doesn’t mistakenly attack the body’s own cells thinking it’s an infectious agent. Immature immune systems need know when to turn off as much as when to turn on.
High Risk of auto-immune disorders
Immune system confusion about chemical signatures on pathogens versus host cells may trigger auto-immune disorders such as diabetes, rheumatoid arthritis and multiple sclerosis. The immune system somehow mistakes self for foreign invaders and attacks specific host cell types, resulting in destruction of native cells.
Finally, natural immunity from infection by one respiratory virus teaches the young immune system to prepare for other types of respiratory viruses that carry similar chemical signatures, and not just variants of a single virus like SARS-CoV-2.
In this way, the adaptive immune system library of defense tools is built and becomes robust and cross-reactive to a variety of threats that have yet to invade.
How COVID-19 vaccine damages young immune systems
Vaccine-generated antibodies, from either maternal transmission of a vaxxed mom to the fetus or from direct childhood immunization, bind tightly to the SARS-CoV-2 spike or S-protein (high affinity). These antibodies outcompete innate system antibodies, but unlike the natural antibodies, they are non-sterilizing.
The child’s immature innate system is prevented from the “training” it needs to learn to identify the spike and neutralize it.
If vaccine antibody generation is constrained by spike (S) protein only, the adaptive system may not build its full defensive library to include responses to all the other viral protein sites which are less likely to mutate.
Viruses contain many proteins the immune system must learn to recognize
COVID-19 virus comprises several proteins that our immune systems learn to recognize. These include four structural proteins, the S-protein which binds to human cell receptors, E- and M-proteins that form the viral envelope, and N-protein that binds to viral RNA.
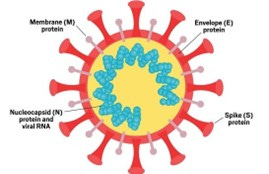
These viral proteins all serve to alert the immune system about the presence of a foreign invader.
If antibodies generated by mRNA vaccines are constrained by responding to the S-protein only, the adaptive immune system may not build its defensive
library to include responses to other coronavirus proteins, some of which are less likely to mutate compared with the S protein.
Also, young constrained immune systems are less likely to mount a robust immune response to other respiratory viruses that carry some of the same protein markers as coronaviruses. This makes children less capable of fighting off common viruses and more likely to develop chronic viral infections.
This constrained development of the immune system is known as Immune Imprinting, also called original antigenic Sin or OAS. OAS will result in several immune system impairments.
Immune Imprinting
Immune imprinting (also referred to as Original Antigenic Sin or OAS, also Immuno-fixation) refers to a phenomenon whereby initial exposure to a viral strain may prevent the body from producing enough sterilizing antibodies against a new strains of the virus.
The immune system is trained to respond to one strain and not related variants.
Immune imprinting increases the infectiousness of the virus to the vaccinated child as well as vaccinated and boosted adults. That is the reason behind rising hospitalizations and deaths due to Omicron variants observed in several highly vaccinated countries, including UK, Israel, the EU, Australia and New Zealand among others.

This is in contrast to countries with low rates of vaccination throughout Africa, India and elsewhere which are not experiencing the same jump in
hospitalizations and deaths. In other words, the Herd is not fixated on one strain.
These countries have developed true herd immunity to SARS-CoV-2 and better able to combat new variants as they emerge.
Conclusion
Vaccination of children with mRNA vaccines designed to elicit an antibody response to only the spike or S protein and not the full array of viral protein markers may impair immune system development during childhood. The consequence of this impairment may be chronic inability to fight off common viruses and other infections.
In light of the statistically zero incidence of severe illness from COVID-19 in healthy children, and the lack of demonstrated safety and effectiveness of childhood mRNA vaccines, parents should carefully consider whether vaccination makes sense for their children.
FLASHBITS:
