
How on earth did the world miss the significance of this data?
How on earth did the world miss the significance of this data?
How on earth did the world miss the significance of this data?

Highlights of this short article;
· Revealing covid-19 mortality data that no one has explained to date?
· Why the extended hypothesis of Robert Edgar Hope-Simpson (REHS) is further supported by this empirical data?
· Why our pandemic response was so fundamentally misguided?
A long while ago I was sent some European excess death data by a guy I follow on Twitter. Excess mortality data enables us to observe trends that provide a reliable perspective on the impact of a pathogen. On receiving this data, I was intrigued by the pronounced and consistent excess mortality dip that was evident prior to the impact of the pandemic. I questioned this with the originator, he did not offer any explanation. At the time I sadly dismissed it. This is a graphical representation of that data;
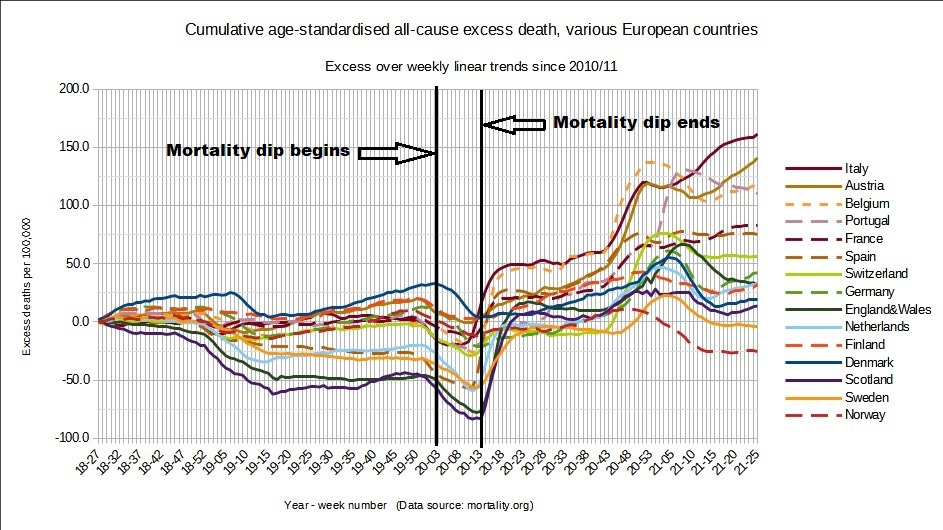
Can the extended hypothesis of REHS explain this data?
For those of you unfamiliar with my previous article(s) (1) this is the extended REHS hypothesis;
Viruses have evolved survival mechanisms using a variety of chemical signals that have evolved over unimaginable number of mutations and time that offer a survival advantage. These chemical signals can emanate from the host, from the virus itself and even from bacteria. In a similar vein the human immune systems operate by a series of chemical signals that have also evolved to recognise and combat a significant pathogen threat.
Covid-19 virus initially embeds at a low / latent level within a significant proportion of the population. The virus infects very rapidly as immune systems are naïve particularly to a “novel” pathogen. Because the prevailing state of the immune systems are relatively blind there is a minimal reaction to the virus during this initial embedding stage.
This minimal human immune reaction relates directly to a chemical signal that the virus will detect and utilise to accelerate the replication cycle, so replication remains at a low level at this stage. Viral embedding and replication may be regarded for this hypothesis as two separate phases.
The embedded virus is then seasonally reactivated by external exposure to specific conditions of UV light. The specific conditions appear twice daily (morning and afternoon) and are enhanced seasonally due to the angle at which the sun’s UV rays penetrate and are absorbed by the atmosphere. Ozone (O3) is one of the primary UV absorbers, but other molecules will also have an impact.
The process of mutation selection is by infected individuals continually exhaling viral mutations at a low level the UV modified viral particles are then inhaled by the host who is in closest proximity to the original exhaled breath. Viruses such as covid-19 continually mutate due to RNA replication errors. The mutations that reach the external environment must have a greater ability to escape the prevailing state of the hosts immune system. Consequently, the immune system is effectively acting as a mutation filter. Conditions that facilitate viral suspension; humidity, temperature and air flow will also be factor as this enables the viral particle suspension near to the host. The viral particles are exposed to the current UV light conditions. If the light is too intense it will destroy the viral RNA but if the light conditions are at a specific intensity this will cleave the RNA which can renter the host cells more readily (2).
The cleaved fragments recombine within the cell. Since the mechanism is selecting cleaved RNA fragments from successful mutations and then recombining it is feasible that this process facilitates selection of even more successful mutations. It is also possible that specific UV light conditions cause minor damage to the RNA which further promotes mutations on recombination and repair within the host cells.
This UV light selection process is a mechanism that has evolved to generate and select mutations that have an advantage to escape the prevailing state of the human immune system. From the hosts standpoint the immune system does not want to activate for a minor viral attack as we would be perpetually sick, so this threshold level based on rate of cell entry has evolved to optimise immune response to only a significant threat.
Healthy immune systems select mutations that have the capacity to rapidly enter the cells of less healthy immune systems. The speed at which cell entry by these selected mutations is occurring in the less healthy immune systems rapidly exceeds the threshold level and consequently they react much more severely. The severity of the immune response is why these individuals have very little infectious potential and why secondary infections are so low for respiratory viruses such as covid-19 and influenza (3).
Clearly external exposure to UV light is required for activation but once activated, a healthy individual is briefly highly infectious in all settings. Their immune systems rapidly deal with the selected mutation(s) so they are sick for only a short period, so they are effectively asymptomatic superspreaders.
Applying this hypothesis to provide an explanation for the above dips in mortality data;
The activating signal is specific seasonally enhanced conditions of UV light which create an increased new infection cycle by selecting a mutation. During the initial cell entry phase there is a degree of pathogen interference (4) which is where a dominant new viral mutation has the capacity, using chemical signalling, to suppress other pathogens including other covid-19 variants. The suppression of covid-19 variants is clearly also a product of the prevailing state of the immune system. This is why influenza and respiratory syncytial virus (RSV) virtually disappeared during the pandemic. This pathogen suppression of other respiratory viruses, which are also seasonally activated, is reflected in the excess mortality data. We must bear in mind that the excess mortality is comparing what is “normal” mortality for that specific time of year. In terms of mortality when the cell infection level is at a consistent threshold level the immune system reacts. The virus also detects, through chemical signalling, this human immune response and counters by accelerating the replication cycle hence the rapid mortality spike. I have examined two regions around the world; South America and Europe to examine if a dip was present and to what extent. This data is represented in the table below (source – Our World in Data);
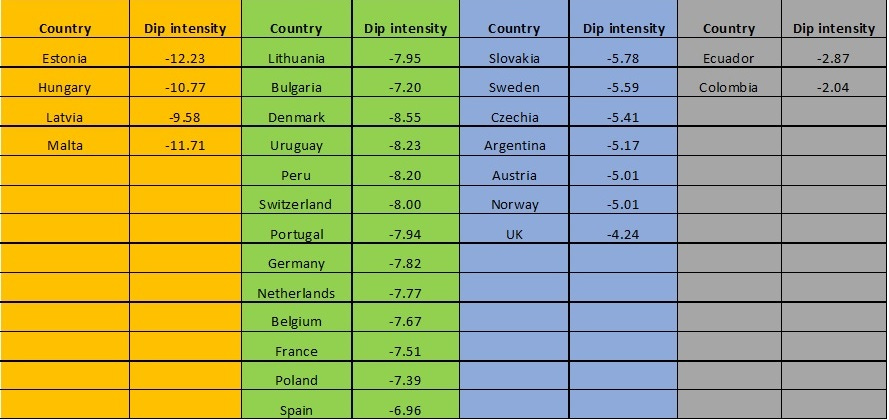
The data appears to be grouped in four clusters with quite consistent mortality dips within those clusters. Why is this occurring? All countries have been included where data was available.
The extended REHS hypothesis is predicated on seasonal selection of more immune evasive mutations. If this is the case, we should be able to see mortality dips occurring seasonally. I have examined the Mortality Watch database for three of the countries examined in the original data. I have also extended the period back to 2016 to examine how exceptional this dip phenomenon is. This data is shown graphically below;
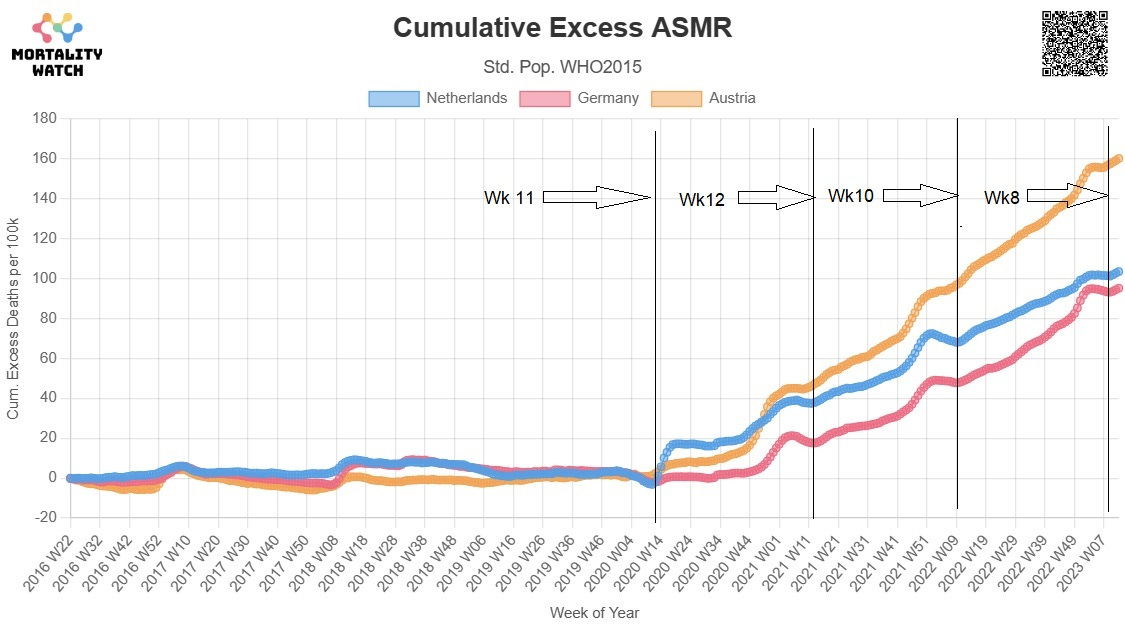
We can see that there are indeed consistent mortality dips occurring at annual intervals for all these three European countries in addition this appears to be quite an exceptional occurrence compared with previous years. This is in keeping with the proposed hypothesis of a newly selected mutation initially embedding within the population and suppressing the impact of other variants through immune response and pathogen interference.
If the above hypothesis is correct, then the pandemic response was clearly misguided. Individuals / superspreaders are triggering simultaneously everywhere and this is supported by the ONS data that I previously provided (1). To summarise that data all 10 regions of England and Wales triggered within a 3 to 4 day window and this was also repeated in Spain plus other regions / countries around the world. Masks will have little bearing if this mechanism is correct as viral particles are far too small for masks to have an impact and superspreaders are popping up randomly and seasonally activated in all locations. Social distancing will have little or no impact because virtually everyone has been exposed and the fundamental problem is the exposure of less healthy immune systems to healthy ones. If we translate this concept to a care home or hospital environment, where we have a significant age difference interaction, we will have a disastrous situation, which is exactly what happened.
From the original data we can established that there is a significant period of around 10 weeks whilst the viral mutation is infecting the population where is nett benefit on mortality. From this it is implicit that the viral mutation had already established itself in a significant proportion of the population. Consequently, track and trace would have little or no bearing on transmission or mortality. Is there any evidence from this data that establishes when the initial infection period commenced? We have stated that the selection period is seasonally activated so let us project back a year to see if a 2019 mortality dip occurred;
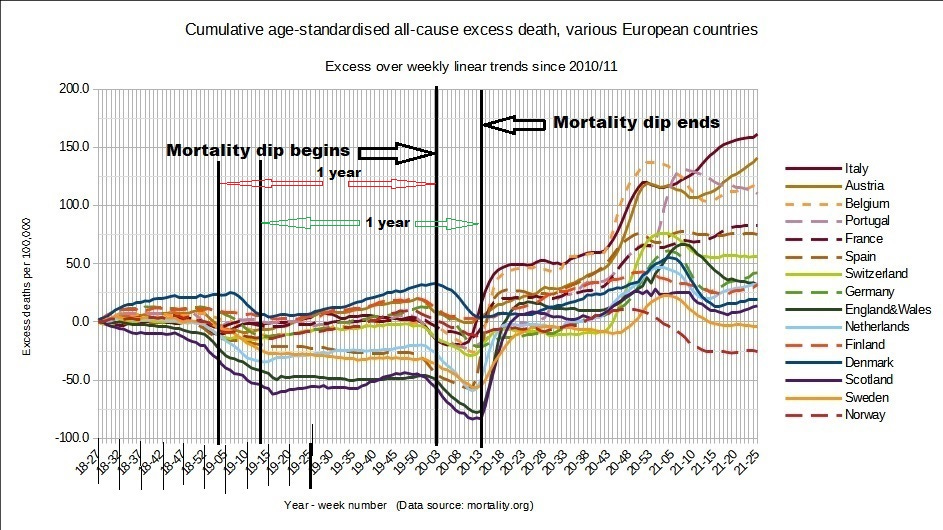
We can see that a similar event occurred in 2019 with virtually all these European countries having a seasonal mortality dip. There is evidence that this dip was slightly more dispersed and variable in intensity. This data may be explained by applying the extended hypothesis outlined above to the concept of a very novel virus entering, in this instance, the European population. As this virus is very novel it can readily evade the prevailing state of the human immune system. During this phase there is a prolonged phase of cell entry / embedding within the population once again we see pathogen interference causing a dip in mortality in virtually all countries. However, the population is relatively immune blind to this selected variant so consequently there is a minor reaction in terms of severe mortality. As the threshold for immune reaction is reached and an immune response is mounted. For a significant number of European countries this results in a nett mortality benefit. However, once the virus has been seasonally cycled through the immune systems on several occasions, mutations
are now being selected that have greater capacity to rapidly evade the less healthy but primed immune systems and cause a more severe immune response resulting in the sudden rise in mortality seen in the second seasonally activated cycle.
As previously mentioned, this is supporting evidence that this is a very novel virus and had significant properties that enabled it to evade the human immune system that strongly indicate gain of function origins. To expand if this if there is a relatively novel virus released in this manner it will not diversify through mutation until it is filtered through the prevailing state of the human immune system and it is not until the this has happened that a rapid cell challenge in the “unhealthy” and corresponding immune response will result in more severe outcomes. Initially the virus is regulating its cell entry at a rate below the threshold level for a significant immune response.
If this is correct, we should be able to see the filtering effect if we examine mutation versus time. We should see intense selection in the more deadly variants of concern (Alpha and Delta) as these are subject to a severe immune response and thus are rapidly selecting mutations that can infect the less healthy at a speed which rapidly activates their immune systems.
Data from the GISAID database (5) is broadly supportive of that concept. If we compare the emergence patterns variants of concern of the most heavily impacted countries with those that are less impacted, we can see a significant difference.
We can also observe that variants followed the same pattern in terms of timing and variant pretty much the same all around the world. This must infer that there is an underlying mechanism for the rate of mutation but the sudden rise of variants of concern is responsible for the severity impact. An alternative concept is that a respiratory virus is a quasi-species (6) that emerges as a cloud of mutations and that that cloud is both focused by the prevailing state of the immune system on mutations that are more capable of evading the immune system. The UV mechanism is selecting and increasing the focus and dominance of a particular class of mutation. If the human immune system is allowed to gradually respond the severity impact is much less. This is in keeping with the proposed extended hypothesis. This is all a result of the constant rate of RNA replication error coupled with the prevailing state of the human immune system and the UV light specific selection process. Where the UV light conditions are prolonged, such as Ecuador and Peru (7) we get a more intense focused emergence of variants because more superspreaders have been activated. They are of course variants of concern (VOC) as they have been selected by the mechanism to evade the immune system. This GISAID data unfortunately does not extend back to the total period of interest as we were not monitoring VOC then. In addition, there is great variation in the level of genomic testing but hopefully the relatively of the peaks particularly during the latter periods of the pandemic will provide evidence.
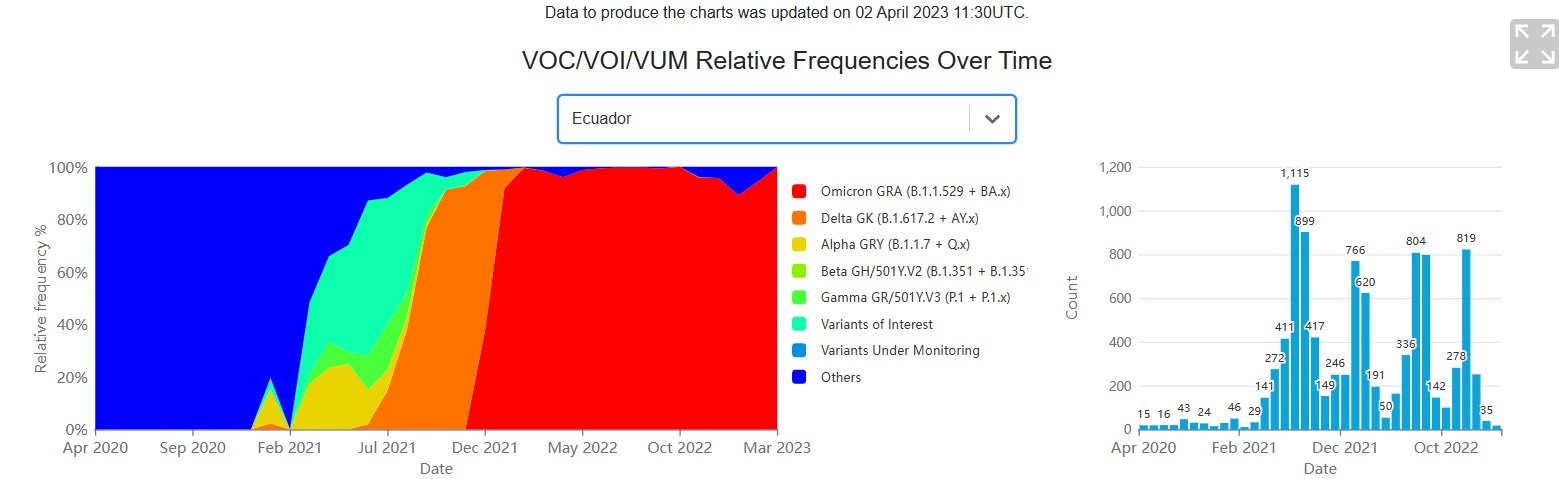
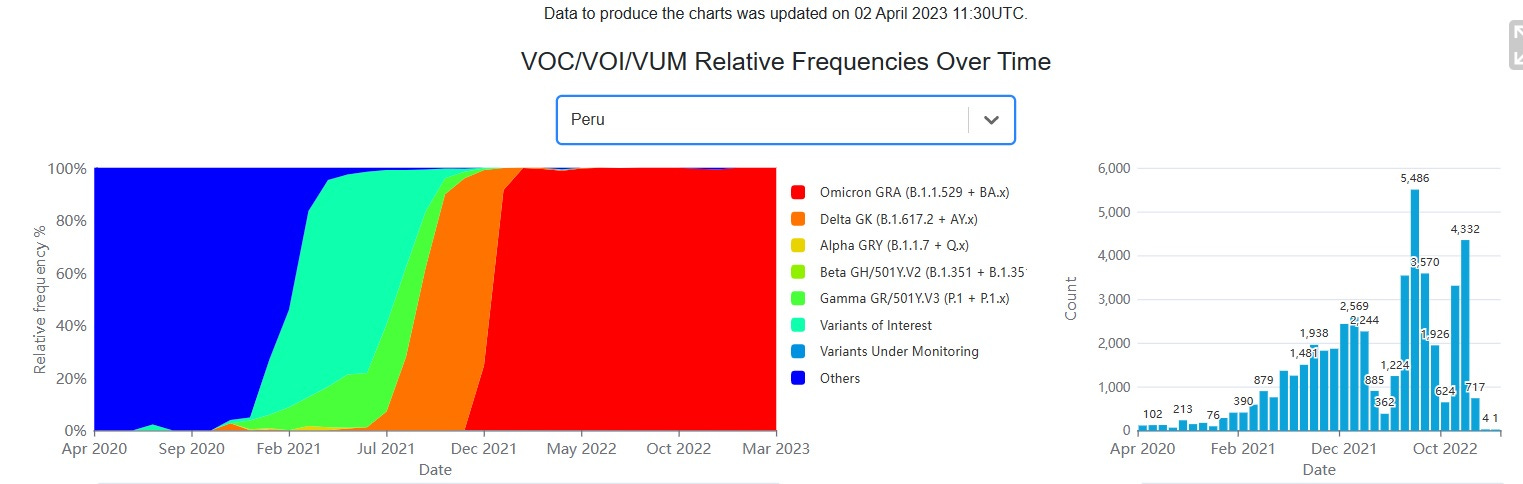
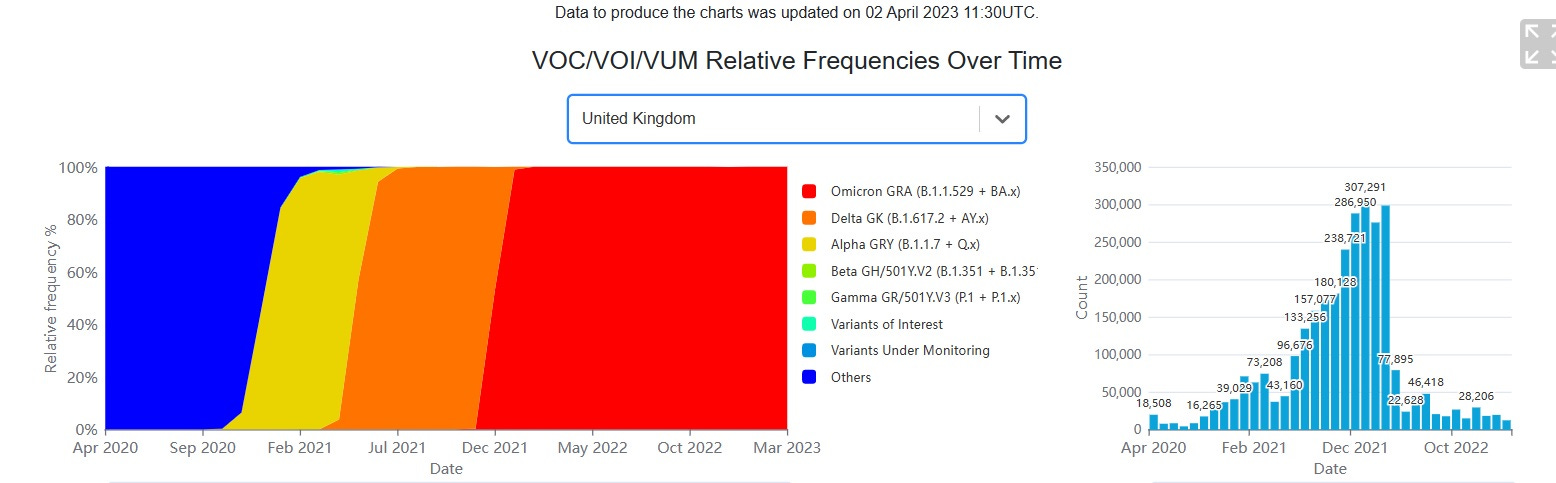
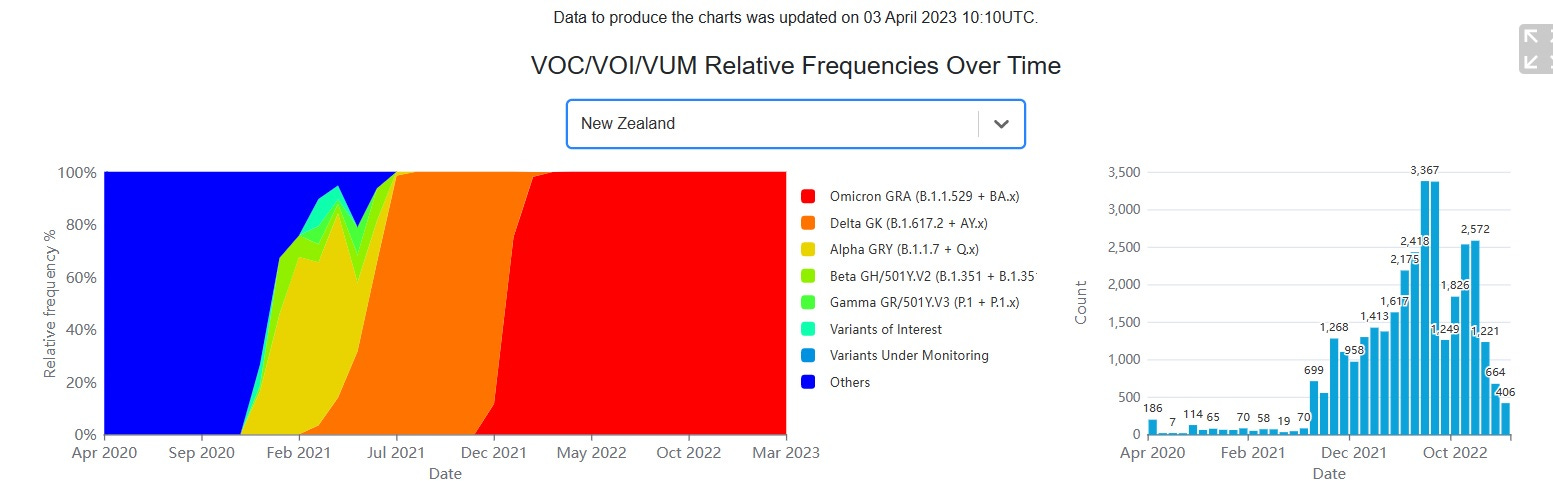
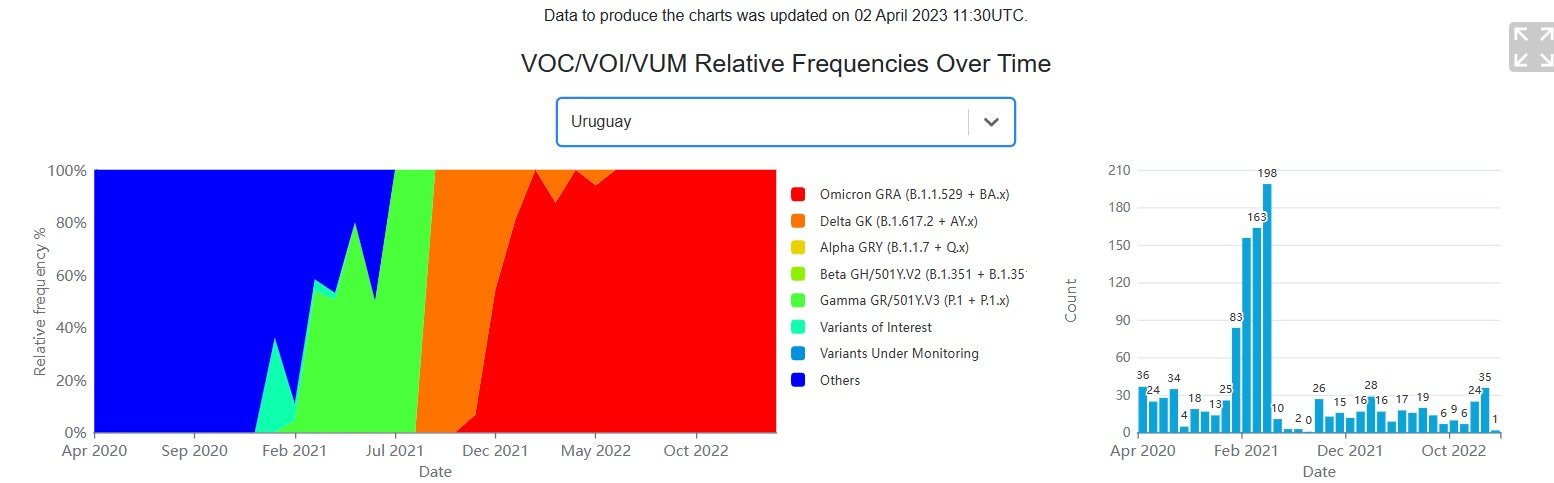
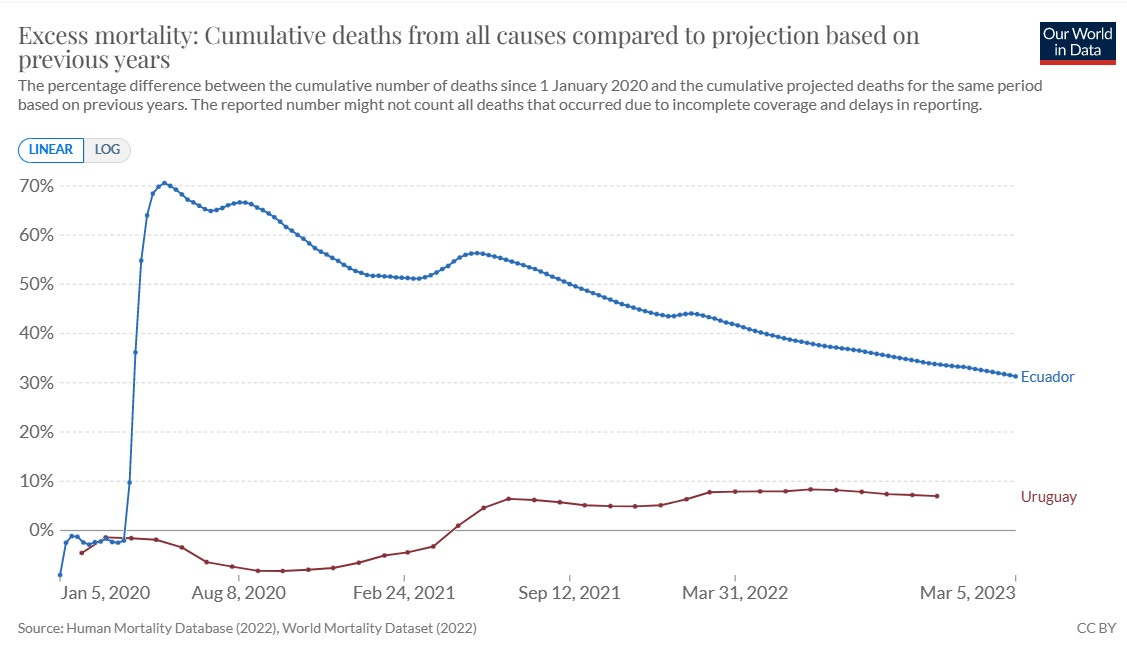
What appears to be occurring from these charts is that countries that were severely impacted experience broadly the same emergence of VOC’s but they are more intense and more variable peaks. This is probably a result of the variant cloud is being focused on mutations that are capable of immune evasion. This gives rise to intense and rapid exposure to unhealthy immune systems in those countries with corresponding severity of reaction and mortality. The mortality response will recede over time due to the removal of susceptible individuals and the specific strengthening of the prevailing state of the human immune system. This is well illustrated by the comparison of Uruguay and Ecuador in the above chart and the chart shown below:
Conclusions
The world chose to ignore the extensive work of Robert Edgar Hope-Simpson (8) and live in a world of fear induced responses that did not remotely align with empirical data. This has led us an untold number of pandemic induced rabbit holes. We have never generated so much data on a respiratory virus. Let us use that information to gain a more accurate understanding so we can react more optimally in the future. If anyone has any “black swans” for this extended hypothesis, please comment. It is how we progress. I think it’s called science.
PS We can do better than a plaque to this great scientist!
References:
1. Were Charles Darwin and Robert Edgar Hope-Simpson right about Covid-19?
https://acrobat.adobe.com/link/review?uri=urn:aaid:scds:US:f7667f08-0134-45d4-9c97-a1a07d01651d
1. Substack (alternative link. Note parts 2 to 6 are on a different Newsletter)
2. UV and violet light can Neutralize SARS-CoV-2 Infectivity
https://www.sciencedirect.com/science/article/pii/S2666469021000920
Relevant text from this paper;
Cell-by-cell distribution of the FISH signal displayed a bi-modal distribution, with 20-40% of cells being clearly infected at 24 hours post infection when non-irradiated virus was seeded on cells (Fig. 5C). In contrast with these data, all the analyzed UV-wavelength reduced the fraction of positive cells, as probed by smFISH, resulting in a complete inhibition of the virus when SARS-CoV-2 was irradiated with wavelength specific critical doses (4mJ/cm2 for UV-C, 200mJ/cm2 for UV-B, 4000 mJ/cm2 for UV-A and 24000 mJ/cm2 for violet light) (Fig. 5D). Notably at lower UV doses some cells with high levels of vRNA could be detected, suggesting that, rather than inhibiting the capability of the viral genome to replicate, UV-irradiation might affect either virus entry in the cells or the assembly of functional viral particles following the replication of the viral genome.
3. Secondary Attack Rates
4. Roles for Pathogen Interference in Influenza Vaccination, with Implications to Vaccine Effectiveness (VE) and Attribution of Influenza Deaths
5. GISAID Link
GISAID - hCoV-19 Variants Dashboard
6. Quasispecies diversity determines pathogenesis through cooperative interactions in a viral population;
https://www.nature.com/articles/nature04388
7. Were Charles Darwin and Robert Edgar Hope-Simpson right about Covid-19? Part 5
8. REHS 1987 joint paper (Full text);
I'd love for you and JJ Couey to put your heads together on this.