

Alternative Eats Part III: Artificial Sweeteners and Cancer
Alternative Eats Part III: Artificial Sweeteners and Cancer
Does consuming artificial sweeteners increase cancer risk?
When it comes to artificial sweeteners, I think a lot of the concern is in the name: people are worried that consuming something artificial will “obviously” have negative impacts on their health.
This is one form of the Appeal to Nature, a logical fallacy where we assume that all things natural are “good” and all things unnatural are “bad”.
Although I do see it come into play a little bit in the conversation around artificial sweeteners and weight management–the last topic we covered in the Alternative Eats Series (I, II, IIa)–I see the Appeal to Nature in action much more often in terms of artificial sweeteners and cancer risk.
But, is this intuitive line of thinking genuinely backed up by studies, or is it mostly misguided?
Here, we’ll dive into that question, covering what artificial sweetener research suggests regarding these compounds and cancer risk.
WARNING: As the Deep End description alludes to, this deep dive content is not for the weary-eyed or faint-minded. You’ve been forewarned, in-depth, nerdy content that will equip you with scientifically-based conclusions regarding artificial sweeteners and cancer lies ahead.
Friendly Disclaimer: I am not a doctor, and none of the information below is medical advice in any way, shape, or form. You are responsible for conducting your own research, consulting your medical professionals, and making your own decisions.
If you want to catch yourself up or revisit the other parts of the Alternative Eats Series, here they are:
Part I: “Kicking Off a Deep Dive Into Artificial and Natural Sweeteners”
Part II: “Exploring the Utility of Artificial Sweeteners For Weight-Loss”
Part IIa: “Covering Two New Studies On Artificial Sweeteners ad Weight-Loss”
(Not So) Brief Tangent on Observational Research
Before we take a look at the data, it’s important to acknowledge a key difference between the artificial sweetener research about cancer and that which we previously covered about weight management.
When it comes to the latter, we have many randomized-controlled-trials (RCTs)—the gold standard of studies–to draw conclusions from; whereas, when looking at cancer, we pretty much don’t have any human RCTs at our disposal.
This is sort of an unavoidable issue with nutritional cancer research, in that it simply isn’t feasible to run an RCT to answer the question, “Does consuming X cause cancer?”. One reason is that this would mean separating two similar groups of people, getting them to eat exactly the same diet except for one group consuming artificial sweeteners, having them follow the same remaining lifestyle habits (i.e. exercise, sleep, smoking, etc.), then following them over a decade and tracking which group develops more cancer.
For reference, if you asked an actual scientist involved in RCT research, I think they would tell you it’s enough work to check these boxes for a study lasting a single month.
For this reason, essentially all of the human research on artificial sweeteners and cancer comes from epidemiology, a flavor of observational research that assesses factors and patterns of health or lack thereof in populations. In the case of artificial sweeteners, this most commonly looks like giving tens of thousands of people a questionnaire regarding their diet and lifestyle in the past year or so, then following up with those people across ~5-20 years and identifying whether people who reported consuming more or less artificial sweeteners were more or less likely to get cancer.
This is important to note because, as I mentioned in a recent post all about observational research, these types of studies come with more than a few grains of salt due to their lack of control, vulnerability to confounding, and inability to show causation.
In other words, due to their design, it’s impossible to deduce that artificial sweeteners cause cancer with certainty. Furthermore, it’s difficult to deduce whether an observed association (i.e. individuals who do “X” tend to get “Y” disease more often) between artificial sweeteners and cancer represents a legitimate relationship that we should be concerned about or if it’s just noise generated by chance observational outcomes.
If you’ve zoned out, fallen asleep, or if I’ve just plain lost you above, the key point is that the data from observational studies is generally less reliable than that from RCTs, which is an issue when you’re trying to draw strong conclusions.
Fortunately for us, in 1965 a British scientist named Austin Bradford Hill proposed a solution to this issue. (XL, XLVIII) He suggested that we could more accurately weigh the strength of observational data by viewing them through the lens of 9 viewpoints known today as the Bradford-Hill criteria (XL, XLVIII):
Strength: How big of an effect is there?
Consistency: Do we see a similar effect across multiple studies conducted by different researchers in different places?
Specificity: Is the association linking a particular cause with a particular effect (ex: consuming a particular artificial sweetener leading to a particular cancer) or is it linking a broad cause with a broad effect (ex: the American diet contains artificial sweeteners and this diet is associated with cancer overall).
Temporality: Does the cause come before the effect? (ex: Are people consuming artificial sweeteners then getting cancer, or are they getting cancer then starting to consume artificial sweeteners?)
Biological gradient: Does more of the cause lead to a greater effect (i.e. dose-response relationship)? (ex: Does consuming more and more artificial sweeteners lead to greater and greater risk of cancer? Does consuming a lot of artificial sweeteners lead to greater risk of cancer than consuming a small amount of artificial sweeteners?)
Plausibility: Is there a biological explanation for the observed outcomes? (ex: Is there mechanistic data in cell cultures and animal studies suggesting that artificial sweeteners cause cancer?)
Coherence: Do the results of observational studies match the results of the entire body of evidence on the topic (i.e. animal models, in-vitro models, randomized-controlled trials, meta-analyses, reviews)?
Experiment: What do experimental studies (i.e. RCTs) show on the topic? (Again, these are widely viewed as the gold standard of research.)
Analogy: Is there a similar compound that shows the same results as seen in observational studies? (ex: Compound “X” shares a similar chemical structure with aspartame. Is there strong evidence that Compound “X” is associated with cancer?)
Notably, none of these criteria are necessary or sufficient–we cannot draw definitive conclusions just because one or any of the criteria are present or absent. Rather, the presence or absence of each can contribute to the zoomed-out argument for or against causation.
If many of the 9 criteria are clearly present, then it’s more likely that an association represents causation; contrarily, if many of the 9 criteria are clearly absent or pointing in the direction of no causation, then it’s less likely that an association represents causation.
“None of my nine viewpoints can bring indisputable evidence for or against the cause and-effect hypothesis and none can be required as a sine qua non. What they can do, with greater or less strength, is to help us to make up our minds on the fundamental question - is there any other way of explaining the set of facts before us, is there any other answer equally, or more, likely than cause and effect?” - Sir Austin Bradford Hill (XLVIII)
With these criteria at our disposal, we can more confidently assess what is otherwise more unreliable observational data. And, with that nerdy, statistical tangent out of the way, we can now get to answering the question we’re here for: what does research on artificial sweeteners and cancer suggest?
Observations On Artificial Sweeteners and Cancer
As I alluded to above, much of the human research on artificial sweeteners and cancer consists of what are called prospective cohort studies. These studies largely entail recruiting a group of tens-to-hundreds of thousands of people, having them fill out some type of questionnaire or 1-day food record, and tracking them across years to decades.
The best versions of these studies have subjects repeat the questionnaires/records throughout the study period (II, VIII), while worse versions solely utilize the data from the first questionnaire/record to represent subjects’ dietary habits for several years or decades. (XXXVII, XLI, XLII, XLIII, XLIV, XLV)
Consider two things here:
How accurately can you recall how much/often you consumed artificial sweeteners or artificially sweetened drinks in the past year? Even less, how accurately can you recall everything you ate or drank in the past week? How about in the past day?
How different is your diet today compared to what it was 10 years ago? How about even 1 year ago?
With these points in mind, it’s easy to see why these studies are less than ideal from an accuracy standpoint.
Nonetheless, they are, by default, the best evidence we have in human studies. So, what do they show?
Strength, Consistency, and Specificity
Based on my deep dive, many of these studies show no association between artificial sweetener consumption and overall cancer incidence or incidence of specific types of cancer. (VIII, X, XI, XIV, XVI, XVII, XIX, XLII, XLIV, XLV)
On the other hand, several studies do show some type of positive association between artificial sweeteners and cancer risk (i.e. suggesting that artificial sweetener consumption is associated with increased cancer risk or cancer mortality), whether that be overall cancer risk or risk of being diagnosed with or dying from a specific type of cancer. (II, III, XII, XIII, XV, XXXVII, XLI)
However, none of these studies show a clinically meaningful increase in absolute risk.
For example, Debras et al. found the following in their 2022 study where they followed 102,865 French adults (average age at baseline: 42.4 years old) for a median of 7.7 years (II):
Overall Cancer Incidence (per total artificial sweetener consumption):
Non-consumers: 3.10% (Reference)
Low Consumers: 3.92% (Hazard Ratio: 1.14)
High Consumers: 3.17% (Hazard Ratio: 1.13)
Obesity-Related Cancers Incidence (per total artificial sweetener consumption):
Non-consumers: 1.9% (Reference)
Low Consumers: 2.28% (Hazard Ratio: 1.08)
High Consumers: 1.89% (Hazard Ratio: 1.13)
Breast Cancer Incidence (per aspartame consumption):
Non-consumers: 1.14% (Reference)
Low Consumers: 1.47% (Hazard Ratio: 1.09)
High Consumers: 1.3% (Hazard Ratio: 1.22)
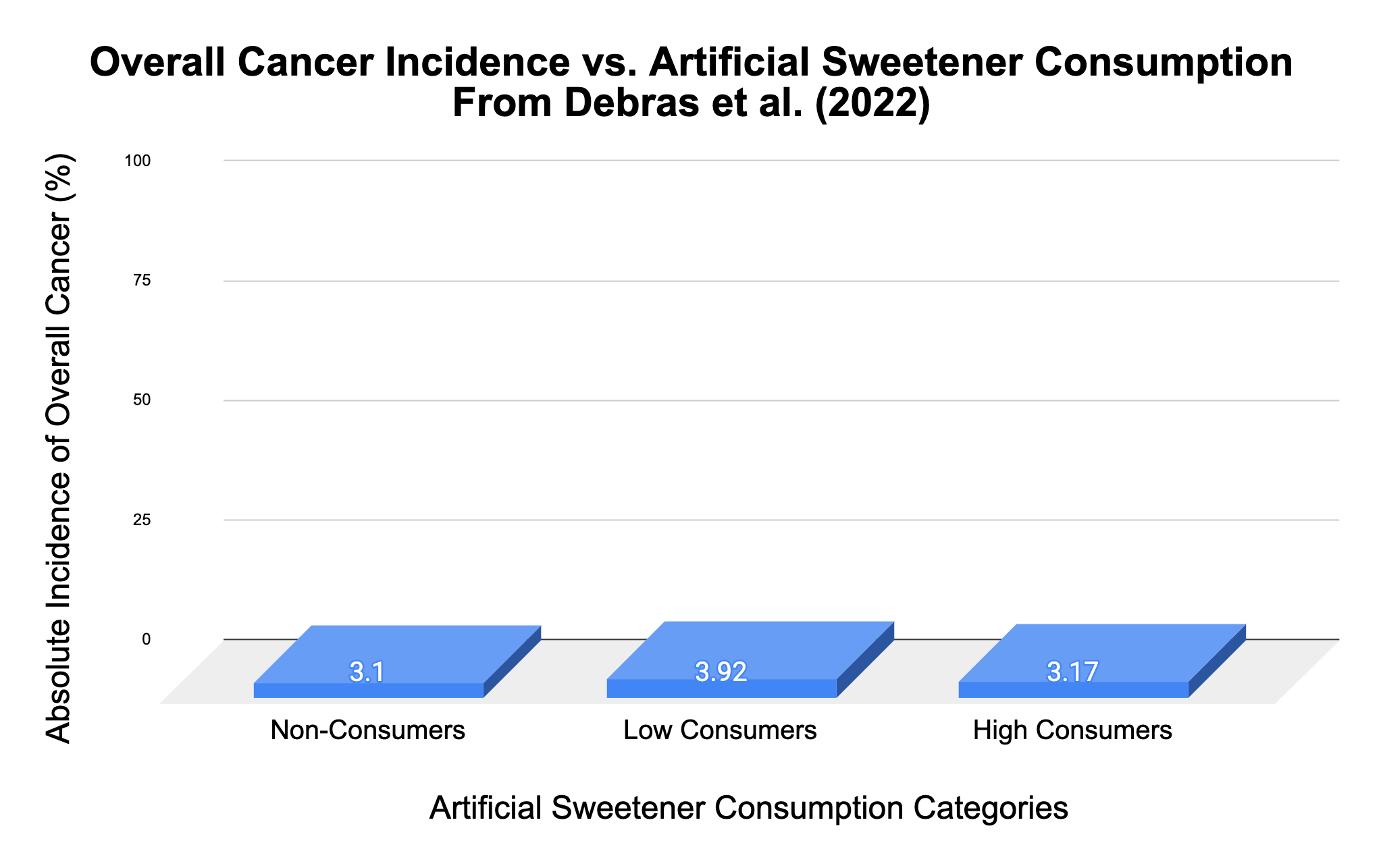
If we return to viewpoint #1 from the Bradford Hill Criteria, it’s clear that the strength of these associations is weak when viewed from an absolute risk standpoint. In other words, the difference of 0.07% in overall cancer risk between non-consumers and high consumers is trivial, especially considering the dodgy reliability of the questionnaires used to obtain these results.
Even in terms of relative risk, the strength of these associations is weak, showing, at best, a 1.22X or 22% relative difference between non-consumers and high consumers (this is shown by the hazard ratios, which are the results after adjusting for confounding variables, like exercise, overall diet, whether people smoke, etc.). And, this is fairly representative of the weak differences in risk you’ll find in the other studies I cited above.
In comparison, the difference in risk of scrotal cancer between chimney sweeps and their co-workers who didn’t sweep chimneys in the late 1700’s–a classic case in the history of epidemiology–was 200X or 19,900% when Percivall Pott concluded that the soot from sweeping chimneys was causing cancer. (XLVIII, XLIX)


Considering that, in addition to the positive associations, numerous studies show no association between artificial sweeteners and cancer, these data are also lacking consistency—viewpoint #2. Not to mention, some studies (III, XXII, XLIII) even show negative associations for certain cancers (i.e. the subjects consuming more artificial sweeteners were less likely to develop/die from cancer in these studies)–though these associations are as weak as the positive findings above.
Furthermore, in terms of consistency, the results are also spurious within the positive studies. For example, McCullough and Colleagues found a trivial increase in pancreatic cancer mortality in their cohort of 934,777 subjects but no association for overall cancer or breast cancer mortality with artificially sweetened beverage consumption after controlling for BMI. (III) In contrast, as shown above, Debras et al. found a trivial increase in overall cancer incidence associated with total artificial sweetener consumption, as well as a trivial increase in breast cancer incidence associated with aspartame consumption. (II)
This inconsistency also ties into lack of specificity, viewpoint #3, as these varied findings do not pin artificial sweetener consumption to a specific type of cancer. This is the case whether we compare studies with different positive findings or if we compare the outcomes of studies that found no associations with those that found positive associations.
Dose-Response Relationship
In addition to lack of strength, consistency, and specificity, these positive findings tend to lack a biological gradient, or dose-response relationship.
For example, in their 19-year study published in 2019, Bassett and Colleagues found a statistically significant positive trend between non-obesity related cancer incidence and artificially sweetened soft drink consumption. (XV)
Non-Obesity-Related Cancer Incidence (per artificially sweetened soft drink consumption):
Never or <1 drink/month: 0.72%; (Reference)
1–3 drinks/month: 0.65%; (Hazard Ratio: 0.96)
1–6 drinks/week: 0.65%; (Hazard Ratio: 0.96)
1 drink/day: 0.77%; (Hazard Ratio: 1.23)
>1 drink/day: 0.81% ; (Hazard Ratio: 1.23)
If there was a dose-response relationship, we would expect to see the risk of cancer gradually increase with greater intakes of artificially sweetened soft drinks across this trend. Instead, we only see statistically significant results for the two groups with the highest consumption (1 drink per day and greater than 1 drink per day). (XV) And, based on the hazard ratios, we don’t see any increase in risk when going from 1 drink per day to greater than 1 drink per day. (XV)

Furthermore, though they aren’t statistically significant, the hazard ratios for 1-3 drinks per month and 1-6 drinks per week show a lower risk of non-obesity related cancer compared with the lowest consumption group (never or less than 1 drink per month). (XV)
The point is that this doesn’t satisfy viewpoint #5 from above, biological gradient. And, the same is generally true for those other studies with positive findings. (II, III, XII, XIII, XXXVII, XLI)
Zooming Out
Importantly, if we zoom out to look at the entire body of evidence, the data remains unconvincing in terms of linking artificial sweetener consumption and cancer.
First, several meta-analyses and reviews–some looking at dozens of observational studies–largely suggest that there is no positive association between artificial sweetener consumption and cancer risk. (IV, V, XVIII, XX, XXI, XXX)
Notably, this includes the World Health Organization’s 2022 meta-analysis by Rios-Leyvraz and Montez, where they found no association between artificial sweetener consumption and overall cancer risk when pooling the results from 39 case-control studies (another type of observational study that’s even less reliable) and 9 cohort studies. (V)
Second, when it comes to in-vitro (i.e. experiments with cell cultures) and animal studies, researchers have largely found that artificial sweeteners are not genotoxic (i.e. cause damage to genes) or carcinogenic, even when using animals that are genetically engineered to be more susceptible to developing cancer and when using high doses of artificial sweeteners. (I, IX, XXIII, XLVI)
There are a few notable exceptions from one lab group where different amounts of aspartame consumption increased the risk of cancer in rats and mice. (XXXII, XXXIII, XXXIV) However, external researchers have criticized the designs and questioned the results of these studies. (XLVI)
In particular, the European Food Safety Authority (EFSA) criticized the unorthodox administration of aspartame across the entirety of these rodents’ lifetimes, suggesting that going beyond the standard of the majority of the rodents’ lifespans leads to inaccurate overestimations of cancer occurrence. (XLVI)
In addition, the EFSA notes that an external pathology group re-assessed the same rodents from these studies and found conflicting results with the original lab group’s cancer diagnoses in some cases. (XLVI)
So, aside from outlier findings from a single lab group that has been brought into question (XXXII, XXXIII, XXXIV), in-vitro and animal models largely suggest there is no mechanistic plausibility for linking artificial sweetener consumption and cancer. (I, IX, XXIII, XLVI)
And, if we pool all of the evidence together to assess the coherence viewpoint, we see that our takeaways from observational studies, meta-analyses, in-vitro studies, and animal models largely point in the same direction: towards no causation.
Experiment, Temporality, and Analogy
In terms of the Bradford Hill Criteria, that leaves us with experiment, temporality, and analogy. Since we already covered RCTs, accepting that there aren’t really any available, we remain with the last two viewpoints.
Being that prospective cohort studies identify artificial sweetener consumption years in advance of identifying cancer outcomes, temporality is one of the criteria that this body of research actually does somewhat reasonably satisfy. Still, as I alluded to above, many studies solely base their findings on baseline questionnaires/records, leaving us to wonder whether the subjects’ artificial sweetener consumptions changed over the years of the study.
And, similar to observational studies on artificial sweeteners and weight management, we still cannot completely rule out reverse causation, or whether individuals developed health issues (i.e. weight gain, type 2 diabetes, etc.) that increased their risk of cancer and then started consuming more artificial sweeteners.
In terms of analogy, we could identify many unnatural or synthetic chemicals that are linked to cancer, though, as I touched on in the intro, this isn’t necessarily a sound argument. From a more specific standpoint, we could actually use analogy to support no causation in some cases, such as for aspartame.
Aspartame is broken down into phenylalanine, aspartic acid, and methanol, each of which is present in greater concentrations in fruits, vegetables, meat, and dairy than what you get from aspartame sweetened foods and beverages. (IX, L)
So, by analogy, if aspartame was strongly associated with cancer, we would expect the same to be true of these foods–though, this wouldn’t be necessary per se. At the least, this analogy example does not strengthen the argument for aspartame causing cancer.
Conclusion
We went over a lot, so let’s zoom out once more and look at this research around artificial sweeteners and cancer through the lens of the Bradford Hill Criteria:
Strength: Observational studies show weak associations in terms of both absolute and relative risk.
Consistency: Outcomes amongst observational studies vary with some studies showing no association, others showing positive associations, and a few showing negative associations. Furthermore, there is variation within the positive findings, in that there are conflicting findings regarding the types of cancer affected.
Specificity: There are conflicting results, with some studies showing positive associations of certain cancers while other studies show no association or even negative associations with the same cancers.
Temporality: Prospective studies generally show artificial sweetener consumption occurring prior to cancer incidence; however, we cannot completely rule out reverse causation.
Biological gradient: In studies that do show positive associations, there is generally a lack of a dose-response relationship.
Plausibility: Other than a few outliers, in-vitro and animal studies generally show no mechanistic link between artificial sweetener consumption and cancer.
Coherence: From a zoomed-out perspective, including observational studies, meta-analyses, reviews, animal models, and in-vitro studies, the body of evidence largely suggests no link between artificial sweeteners and cancer.
Experiment: Human RCTs are not available on the topic.
Analogy: When considering the breakdown products of aspartame are present in higher quantities in common foods, the link between aspartame and cancer is likely weakened.
In my opinion, at the end of the day, we really don’t have terrific evidence to go off of. Not only are we missing RCTs in this body of evidence, but the observational studies at our disposal are particularly concerning, considering the lack of accuracy and reliability that comes with food questionnaires and dietary records.
With that said, looking at the evidence we do have, I think the argument that artificial sweeteners cause cancer is very weak. In particular, the large amount of studies showing no association and the extremely weak differences in studies that do show an increase in risk give me confidence that I don’t need to worry about these compounds and cancer risk.
What do you think? Did reading this change your mind or strengthen your opinion? Are you still cautious when it comes to artificial sweeteners, or do you use them regularly? I’m curious what you think and glad to share thoughts in the comments.
P.S. Is it a ridiculous idea to subscribe for more science-based health and fitness content like this for FREE?
If not, hit that subscribe button below.