

WHO Said What? Part II
WHO Said What? Part II
Taking a Closer Look at the World Health Organization's Non-sugar Sweetener Data
In Part I of this series, we covered the World Health Organization’s (WHO) updated guidelines on using non-sugar sweeteners (NSSs ; i.e. artificial sweeteners) for weight-loss. Here, I’ll explain a few things I agree and disagree with regarding the WHO’s stance, particularly their assessment of the randomized-controlled trial (RCT) data.
Friendly Disclaimer: I am not a doctor, and none of the information below is medical advice in any way, shape, or form. You are responsible for conducting your own research, consulting your medical professionals, and making your own decisions.
One of the WHO’s main critiques of the RCT data is that the study designs were inconsistent, and I agree. Of the RCTs assessed in Rios-Leyvraz and Montez’s meta analysis, there were variations in terms of the intervention (i.e. NSSs in the form of drinks, foods, pills, or some combination), the duration (i.e. short-,mid-, and long-term), control (i.e. placebo/nothing, water, attention-control, or sugar-sweetened options), and objective (i.e. using an intentionally reduced-calorie weight-loss diet or not).
And, I agree that most of these RCTs were not designed well to answer the following question, “Are NSSs useful for weight-loss?”
But, what would a study that is properly designed to answer this question look like? In my opinion, it would be of mid- (2-6 months) to long-term (6 months+) duration and involve an intentional weight-loss or weight-loss maintenance protocol including NSS-use or substitution for caloric sweeteners (i.e. added sugar). This would provide evidence as to whether or not NSS-use, either as a deliberate sugar substitution or an addition to the diet to manage cravings, is useful in the context of a reduced-calorie, weight-loss diet over time.
When I parsed through the 32 RCTs that Rios-Leyvraz and Montez used for their weight-loss data in their meta-analysis, only 4 of them (less than 15% of the included studies) met this criteria. (VIII, X, XII, XIII) Two of these studies (VIII, X), were weight maintenance follow-up studies that tracked subjects who first participated in weight-loss studies. (IX, XI). Though they were not included in the meta-analysis calculations, even if we add those weight-loss studies, that brings us to only 6 RCTs that meet our design standard.
There were 6 additional studies that I could not get full-text access to; however, according to the information available in their abstracts, 3 do not meet our criteria (XIV, XV, XVI), 2 meet our criteria (XVII, XVIII), and 1 does not provide sufficient details to determine if it meets our criteria (XIX).
So, what do the studies that are properly designed to assess the efficacy of NSS-use for weight loss show?
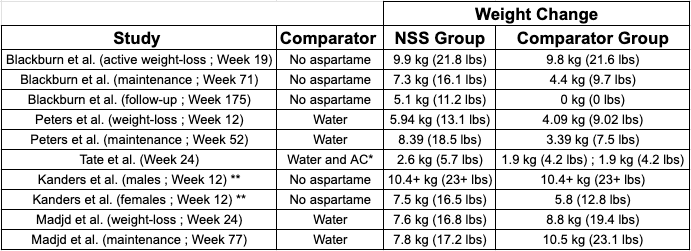
Looking at Table 1, I have two main takeaways:
The NSS groups performed better or similarly to the comparator groups in almost every case.
The subgroup analysis comparing NSS and water groups from Rios-Leyvraz and Montez’s meta-analysis can easily be misinterpreted.
The one slight exception to Takeaway #1 is the maintenance period of the second Madjd et al. study, where the water group achieved ~6 lbs more weight-loss at the close of the maintenance period. (VIII) However, even there, the NSS group still lost a whopping 17.2 lbs on average. (VIII)
And, the results from both Peters et al. studies are reversed, in that the NSS group lost statistically significantly more weight than the water group. (X, XI) Importantly, in both the Madjd et al. and Peters et al. studies, all groups lost significant amounts of weight. To me, this suggests that both the NSS and water protocols were successful, just some more than others in each case–which brings us to Takeaway #2.
One of the WHO’s major claims regarding the RCT data is that NSSs did not show any effect when compared to water. (II) This is true in terms of the statistical results of the meta-analysis, where there was no statistically significant difference between the amount of weight lost by the water and NSS groups. (IV) However, similar to how the WHO believes the RCT data as a whole doesn’t paint a realistic picture of NSS-use for weight-loss, I don’t think these numbers comparing NSS to water tell the whole story.
In particular, the meta-analysis solely compared the differences in weight change between NSS groups and water groups. (IV)This is problematic in isolation because it doesn’t take absolute weight-loss into account–another example of why relative vs. absolute comparisons are important in research statistics.
If you’re interested in learning more about the importance of relative vs. absolute differences in research statistics, check out my posts here and there.
In other words, subjects in the NSS group could lose a significant amount of weight on average but appear to be unsuccessful if they lost less weight than subjects in the water group did on average. For example, as I pointed out above, the NSS group lost statistically significantly less weight during the maintenance period in the second Madjd. et al. study as compared to the water group (~0.4 lbs vs. ~3.7 lbs). (VIII) But, it’s difficult to conclude that the NSS group was unsuccessful on the weight-loss protocol, as they achieved an average weight-loss of 17.2 lbs at the end of the maintenance period as compared to their baseline weight. (VIII)
If we take this perspective into account, rather than interpreting the findings to show that NSS-use is not useful for weight-loss, it appears that both NSSs and water protocols are quite efficacious for losing weight.
Conclusion
The WHO’s guidelines agree with my review of artificial sweeteners and weight-loss in terms of what the hard data show: RCTs suggest NSSs are useful for weight-loss, while observational data suggest they are harmful.
And, I agree with the WHO’s supposition that most of the RCTs are not properly designed to assess whether NSSs are useful for weight-loss in real-world conditions and over mid to long periods of time.
However, I feel the quantity and quality of data from the properly designed RCTs above is still more convincing than that from observational data that are vulnerable to confounding variables, especially reverse causation. And, I think I’ve made a strong case for that here.
But, if we really want answers from an N=1 perspective (i.e. changing the question to “Are NSSs useful for weight-loss FOR ME), I think we can make things much simpler than picking sides over what the data does or doesn’t mean: simply try using NSSs for weight-loss and see what happens.
Of course, you can always just cut calories without using NSSs and lose weight that way as well.
IMPORTANT: If you enjoyed or found this post useful, leave a like and/or a comment to let me know. This will help me gear future content towards what is best for you. Thanks again for reading/listening.