

WHO Said What? Part I
WHO Said What? Part I
Breaking Down the World Health Organization's Guidelines on Non-nutritive Sweeteners
In a recent post, I unraveled my findings from diving into the research literature surrounding artificial sweeteners (AS) and weight management. Amongst my citations for that review were both the World Health Organization’s (WHO) updated guidelines regarding using AS for weight-loss and the meta-analysis off of which those guidelines were based. On the surface, the WHO’s analysis of the data seems to directly oppose my own; however, a little investigation reveals that it’s our interpretation of what the data means for real-world application, rather than our analysis of the data itself, that differs.
Below, I’ll break down their findings, and in a follow-on post I’ll cover aspects where I agree and disagree with their ultimate conclusion that AS are not effective for weight-loss.
Friendly Disclaimer: I am not a doctor, and none of the information below is medical advice in any way, shape, or form. You are responsible for conducting your own research, consulting your medical professionals, and making your own decisions.
Back in 2015, the WHO published new guidelines recommending that individuals limit their intake of free sugars due to negative impacts on body weight and dental caries (i.e. cavities). (I) Since then, they observed an uptick in the use of non-sugar sweeteners (NSS; i.e. artificial sweeteners) as a tactic to reduce free sugar consumption. For this reason, starting in 2016, they began a review of the evidence surrounding how NSS -use impacts body weight and risk of developing non-communicable diseases (i.e. cardiovascular disease, cancer, Type 2 Diabetes, etc.) with the intent to publish guidelines on the topic. (II)
Specifically, they focused these guidelines solely on, “all synthetic and naturally occurring or modified non-nutritive sweeteners that are not classified as sugars,” which, per their definition, does not include sugar alcohols, such as erythritol. Their definition does include common artificial sweeteners, like acesulfame potassium (ace-K), aspartame, advantame, cyclamates, neotame, saccharin, sucralose, stevia, and stevia derivatives.
The WHO initially planned to base their guidelines off of a systematic review by Toews et al. (III); however, since that original systematic review did not contain a sufficient number of studies, the WHO utilized a second systematic review by Rios-Leyvraz and Montez to construct their guidelines. (IV)
This second systematic review contains an abundance of data, including that from 50 randomized-controlled trials, 97 prospective cohort studies, and 47 case-controlled studies, regarding weight-loss and related metrics and non-communicable disease risk in adults and children, as well as outcomes relevant to pregnant women. Here, we’ll mainly take a look at the weight management data.
Similar to what I found in my review, this meta-analysis generally shows that the RCT data suggests NSS-use leads to weight-loss (mean difference of 0.71 kilograms), while the observational data links NSS-use with increased BMI (mean difference of 0.14 kg/m2) and greater risk of obesity (hazard ratio of 1.76, which equates to a 76% increase in relative risk). (IV) They also found that any decreases in body weight were the result of reduced calories following NSS substitution/consumption, rather than any special weight-loss properties of NSS independent of calorie consumption.
So, we generally agree in terms of the objective numbers. Where our conclusions deviate is in the interpretation of those numbers.
While I favor the RCT data, concluding that NSS-use is an effective option for weight-loss, the WHO sided with the observational data in their guidelines, citing, amongst other criticisms, short study duration and indirect design as major flaws in the RCT data. In other words, they feel that, in general, the RCTs looking at NSSs for weight management are too short to support NSS-use. In addition, they feel that many of these studies are poorly designed to answer the question of whether replacing free sugars with NSSs in real-world conditions is effective for weight-loss, in that many of these studies involve adding free sugars to the non-NSS group’s diet on top of adding NSS to the experimental group’s diet.
Also, they cite the following regarding subgroup analyses, where the data was parsed into different study designs:
“When NSS were compared with nothing/placebo or water (i.e. one group in a trial received NSS, and another group received nothing/placebo or water), no effects on body weight or BMI were observed…
…[Also] when NSS were assessed specifically as replacements for free sugars in a small number of RCTs (i.e. habitual consumers of foods or beverages containing free sugars were asked to switch to versions containing NSS in place of free sugars), the effect on body weight was significantly weakened relative to that observed for NSS used in any manner, and an effect on BMI was no longer observed.” (II)
Of note, the authors did recognize the issue of reverse causation–the idea that individuals might consume more NSS because they are overweight/obese and trying to reduce calorie intake, rather than the NSS consumption causing these individuals to become overweight/obese–with regards to the observational prospective cohort data. However, when assessing the data, they felt that, “Most authors of the included studies appreciated the potential role of reverse causation and/or confounding by body weight, and made efforts to minimize the contribution these factors may have made to the results of their studies.” (II)
In other words, they feel that, through tactics like adjusting for confounding variables in their statistical analyses and excluding outcomes from the early years of follow-up where the data may be particularly susceptible to reverse causation, the prospective cohort study authors sufficiently accounted for reverse causation in their study designs.
Importantly, the WHO categorized their ultimate conclusion, “that non-sugar sweeteners not be used as a means of achieving weight control or reducing the risk of noncommunicable diseases,” (II) as a conditional recommendation, as opposed to a strong recommendation. What do these categories mean? Here are the WHO’s definitions:
“Strong recommendations are those recommendations for which the WHO guideline development group is confident that the desirable consequences of implementing the recommendation outweigh the undesirable consequences. Strong recommendations can be adopted as policy in most situations.”
“Conditional recommendations are those recommendations for which the WHO guideline development group is less certain that the desirable consequences of implementing the recommendation outweigh the undesirable consequences or when the anticipated net benefits are very small. Therefore, substantive discussion amongst policy-makers may be required before a conditional recommendation can be adopted as policy.” (II)
So, though it’s clear to me that the WHO is not in favor of using NSS for weight management purposes, their choice of a conditional recommendation suggests that they have lower levels of confidence in this stance. I think this is important to acknowledge, as not doing so can mislead us into extremism and closed-mindedness.
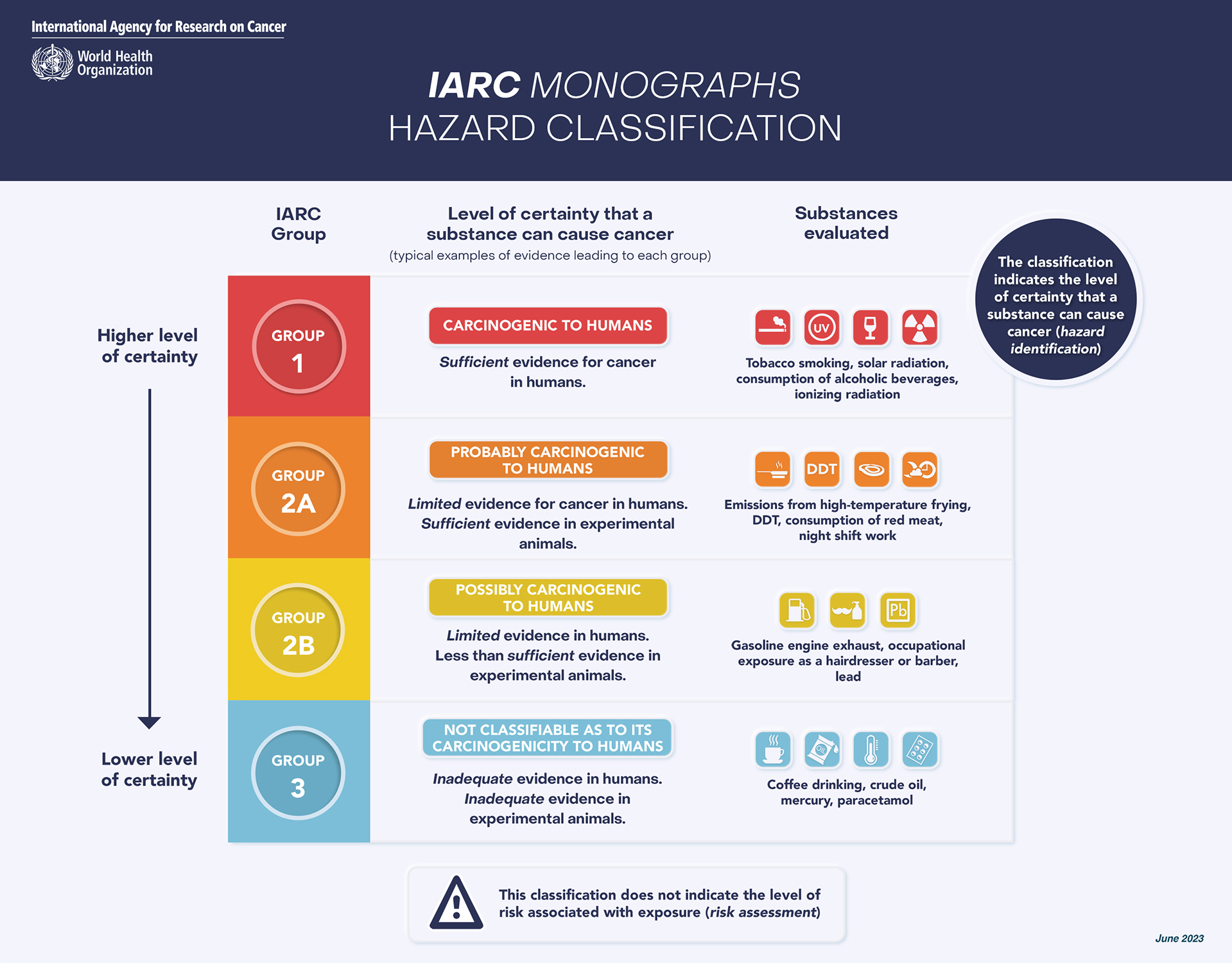
For example, I saw an uproar on social media when the International Agency For Research On Cancer (IARC)–a part of the WHO focused on cancer–labeled aspartame, a popular artificial sweetener, as a Group 2B carcinogen. (V) But, if we look beyond the headline, Group 2B is also called, “Possibly Carcinogenic to Humans,” and is defined by, “limited evidence in humans…[and] less than sufficient evidence in experimental models.” (VI) To put things into perspective, though there are many scary sounding chemicals on the Group 2B list, amongst them there’s also aloe vera and pickled vegetables (“traditional Asian”)–and aspartame. (VII) Yet, all anybody seemed to see was the word, “carcinogen,” after which they essentially equated aspartame with cigarettes.
{kind=link}
Anyways, despite coming to similar conclusions about what the data show, in terms of numbers, the WHO and myself reached different conclusions regarding what the data mean, in terms of interpretation. In Part II on this topic, I’ll explain a few areas where I agree and disagree with the WHO’s stance.
IMPORTANT: If you enjoyed or found this post useful, leave a like and/or a comment to let me know. This will help me gear future content towards what is best for you. Thanks again for reading/listening.