

Abilify IV: Akathisia
Abilify IV: Akathisia
an intense sensation of unease or an inner restlessness that results in a compulsion to move

The Frontier Psychiatrists is a daily health-themed newsletter. For the past few days, I’ve been writing a series about the drug Abilify. That is the first article! The others are…
Abilify III: Bipolar Depression
Today, I’m writing about a common adverse effect of Abilify (aripipiprazole), and other antipsychotics, that is awful to experience. It’s called akathisia, and it’s a neurological syndrome that is a side effect of antipsychotic medications.
The experience is hard to explain, to people who haven't been through it. To people who have experienced it, even if they don’t know what it was, it is unforgettable. Imagine going to the most dreadful movie you’ve ever experienced—if Michael Bay re-made an Inconvenient Truth—and being forced, with a gun to your head, to not move an inch. Imagine being forced to listen to some tech bro mansplain Bitcoin, and having to smile, motionless, the whole time…if you were secretly Satoshi Nakamoto. Now take those feelings, and move them away from the world of words, into your legs. Have to move them. Have. to. move. them.
The horrible part of this inability to remain motionless is that the movement doesn’t scratch the itch very well. People who experience akathisia will pace back and forth, but it never really feels better. It just feels like you have to keep at it:
In most cases the movement is repetitive. The individual may cross, uncross, swing, or shift from one foot to the other. To the observer, this may appear as a persistent fidget
Feeling like you have to move might not sound too bad, but I promise—as someone who has lived this experience—it’s the kind of indescribable nagging awfulness that would haunt your dreams.
It is most commonly associated with antipsychotic medications but can occur with antidepressants as well, and most often rears its ugly head when the dosage is increased rapidly. It can also occur spontaneously in individuals with Parkinson’s disease, which shares pathophysiology with dopamine-blocking drugs. A historical perspective starts with its initial description in 1901 by Dr. Haskovec, who:
concluded that the disorder was of hysterical origin.
In 1975, Van Putten reviewed the early literature on the syndrome:
Bing described it as a “psychosis” characterized by a “morbid fear of sitting down,” but in another chapter he ex- plained it as a way of overcoming the muscular rigidity of Parkinson’s disease. Oppenheim considered akathisia as a form of neurosis, “usually a form of phobia.” Wilson designated it “hysterical” in one chapter of his classic textbook, but he also described the syndrome in association with Parkinson’s disease in a later chapter.
Even physicians had a very hard time comprehending this largely internal experience, which, if not diagnosed, is often disregarded or not addressed as anything other than “anxiety” —Van Putten continues:
patients often are unable to distinguish between anxiety and restlessness, and he warns that “indications of anxiety-like symptoms” such as “uneasiness,” “hy- peractivity,” “pacing, ” “vague complaints about medication,” and “insomnia” may be subtle reflections of akathisia.
His “Many Faces of Akathisia” is a must-read for psychiatrists.1
Much to my surprise, another pivotal article on the topic was authored by a mentor, John M. Kane. He notes that the incidence in individuals treated with dopamine receptor antagonists is between 21-75%, with a prevalence of 20-35%.2 Thus, it happens, to some degree, to many to most individuals treated with these drugs.
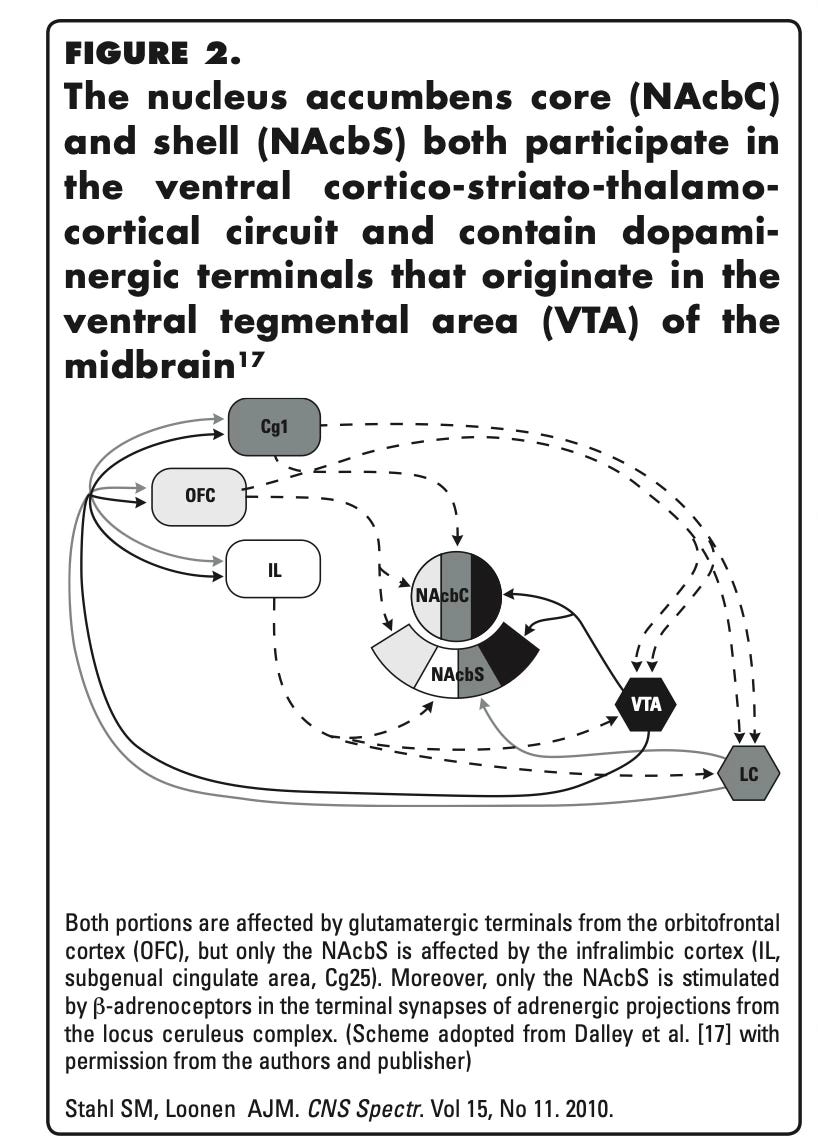
The mechanism is complex and has to do with the role of dopamine in the brain structure we generally think of in terms of addiction and pleasure—the nucleus accumbens (NA).
The NA has a core and a shell, and the neurons in these areas are responsible, as worked out in animal models, for influencing behavior in distinct ways. The shell, according to Stahl and colleagues:
facilitates new behavior that is not necessarily rewarding, but could lead to improvement of the individual’s condition.
Whereas the core is involved in learning to seek pleasurable experiences more:
"preferentially involved in response-reinforcement learning”
Both the core and the shell of the NA are dopaminergic, and dopamine-blocking drugs are what is causing akathisia, thus:
When an individual is compensating for this deficiency by…increasing the adrenergic input from the brainstem, only the [NA Shell] is stimulated. This motivates individuals to display, seemingly purposeless, immediate reward-seeking behavior, and results in activation of the corresponding re-entry circuit.3
So thanks to dopamine blockade, we get a feedback loop that promotes behavior that looks like, to use some slang, “jonesing.” It’s all the drive of someone addicted, and searching for the next “hit,” but none of the pleasure when the activity is carried out. Importantly, there is also none of the explanatory power of being interested in something, anything, much less a high. It’s wanting to go get high…absent wanting and having gotten high, or the promise of pleasure or reward. In a brain circuit, it’s a glitch, most often caused by a medicine.
Those medicines are often prescribed to people who are, well, not always viewed as “reliable reporters.” Their attempts to describe the indescribable are often dismissed. This is why I am taking the trouble to describe the condition, so more people can know what it is, that it exists, and to not ignore it. It is not harmless—this purposeless but relentless restlessness is a risk factor4 for death by suicide5:

There is some data that the association between akathisia and suicidality is stronger in men than women and stronger in new-to-antipsychotic exposed individuals, as well as the severity of depression6
Pearson correlation analysis revealed a significant and positive correlation between akathisia and severity of depression using the modified CDSS-sum score (mCDSS) (Pearson R = 0.404, p < 0.001; Spearman rho = 0.357, p < 0.001), and between akathisia and the suicidality item of the CDSS (Pearson R = 0.388, p < 0.001; Spearman rho = 0.394, p < 0.001).7
Akathisia: it sucks, it’s caused by dopaminergic dysfunction, and, tying this article into my prior articles on Abilify, it’s common in aripiprazole, but it’s also common in other newer antipsychotic medicines like asenapine and lurasidone8:

Keep an eye out, titrate slowly upwards, and don’t dismiss as “anxiety” what could be an adverse effect of a medicine.
Prior articles about medicines in the newsletter include hits like…
Effexor, Buspar, Risperdal, Zyprexa, Neurontin, Xanax, Klonopin, Paxil, Prozac, Clozaril, Lamictal, Lithium, Latuda, Ambien, and generally Benzos, specifically maybe Benzos leading to death by suicide, Geodon, Zoloft, Auvelity.
Please consider becoming a paid subscriber!
Van Putten, T. (1975). The many faces of akathisia. Comprehensive Psychiatry, 16(1), 43-47.
Kane, J. M., Fleischhacker, W. W., Hansen, L., Perlis, R., Pikalov III, A., & Assunção-Talbott, S. (2009). Akathisia: an updated review focusing on second-generation antipsychotics. Journal of clinical psychiatry, 70(5), 627.
Loonen, A. J., & Stahl, S. M. (2011). The mechanism of drug-induced akathisia. CNS spectrums, 16(1), 7-10.
Bjarke, J., Gjerde, H. N., Jørgensen, H. A., Kroken, R. A., Løberg, E. M., & Johnsen, E. (2022). Akathisia and atypical antipsychotics: relation to suicidality, agitation and depression in a clinical trial. Acta Neuropsychiatrica, 34(5), 282-288.
LARACH, V. W. (2001). Relationship between antipsychotic-induced akathisia and tardive dyskinesia and suicidality in schizophrenia: impact of clozapine and olanzapine. Acta psychiat. belg, 101, 128-144.
Bjarke, J., Gjerde, H. N., Jørgensen, H. A., Kroken, R. A., Løberg, E. M., & Johnsen, E. (2022). Akathisia and atypical antipsychotics: relation to suicidality, agitation and depression in a clinical trial. Acta Neuropsychiatrica, 34(5), 282-288.
(the Spearman and Pearson references are to statistical tests)
E Thomas, J., Caballero, J., & A Harrington, C. (2015). The incidence of akathisia in the treatment of schizophrenia with aripiprazole, asenapine and lurasidone: a meta-analysis. Current neuropharmacology, 13(5), 681-691.
I have heard tales of inexperienced prescribers mistaking akathasia for tardive dyskinesia and adding Ingrezza of all things. If that's indeed going on it's safe to say akathasia is poorly recognized and understood. (It does sound really awful--like restless legs syndrome but for your soul.)
Good article. I liked “A Guide to the Extrapyramidal Side-Effects of Antipsychotic Drugs” by DG Cunningham-Owens bitd (fwiw).