

Benzos (benzodiazepines) Are Associated With Death By Suicide.
Benzos (benzodiazepines) Are Associated With Death By Suicide.
Distressing findings about Ativan, Xanax, Klonopin and other common medicines, in an era of increasing risk.

The Frontier Psychiatrists is a daily health-themed newsletter. Today, I bring you the disturbing data on benzodiazepine medications as a follow-up to “hit” articles like Klonopin, Xanax, and Benzos!, previously.
As usual, when scientists look at large data sets, we are indebted to our European colleagues and their comprehensive national health system databases—this one was from France.
Risk of suicide attempt and suicide associated with benzodiazepine: A nationwide case-crossover study
This study looked at the same individuals as their own controls—a powerful statistical approach, and compared:
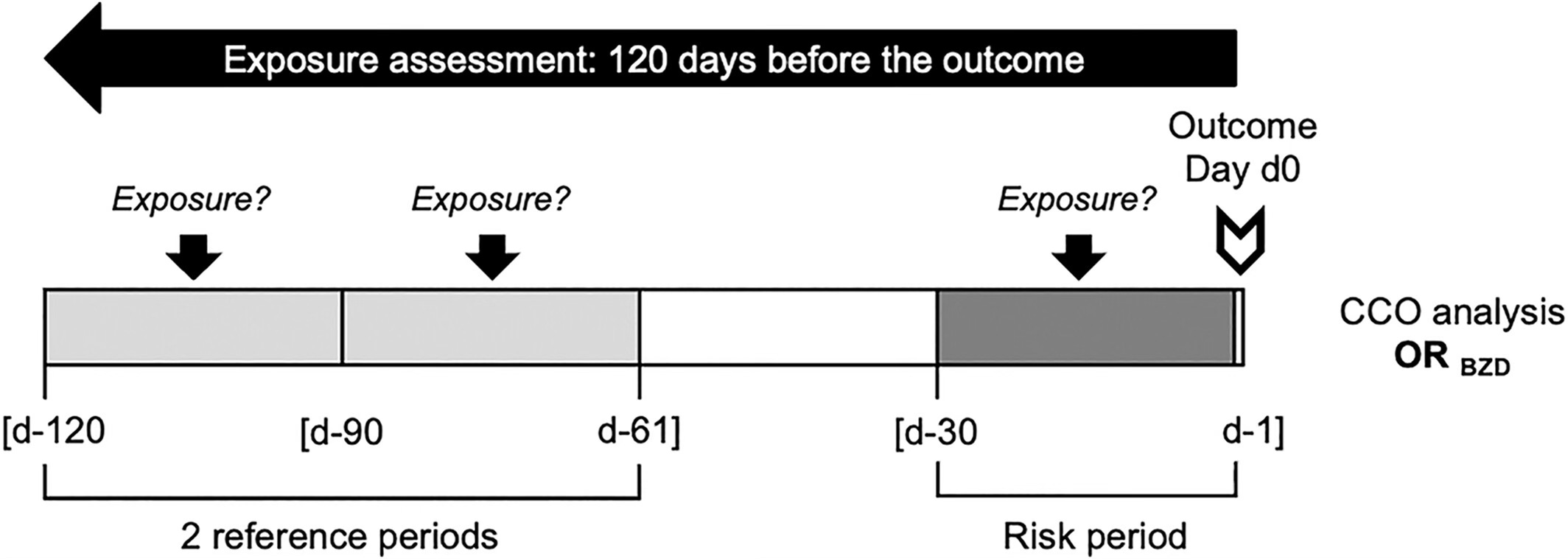
Patients ≥16 years, with hospitalized suicide attempt or suicide between 2013 and 2016, and at least one benzodiazepine dispensing within the 120 days before their act….For each patient, frequency of benzodiazepine dispensing was compared between a risk period (days −30 to −1 before the event) and two matched reference periods (days −120 to −91, and −90 to −61).1
They found:
A total of 111,550 individuals who attempted suicide and 12,312 suicide victims were included, of who, respectively, 77,474 and 7958 had recent psychiatric history.
The relationship to benzo prescribing was as follows (recall, a higher odds ratio is bad in this case, meaning suicide is more likely with benzos prescribed):
Benzodiazepine dispensing appeared higher in the 30-day risk period than in reference ones. The comparison yielded adjusted odds ratios of 1.74 for hospitalised suicide attempt (95% confidence interval 1.69–1.78) and 1.45 for suicide (1.34–1.57) in individuals with recent psychiatric history, and of 2.77 (2.69–2.86) and 1.80 (1.65–1.97) for individuals without [recent psychiatric history].
This is particularly surprising because individuals were not only more likely to attempt or die by suicide if there was a correlated benzodiazepine exposure, but the risk was higher in those without established psychiatric history than in those with a psychiatric history. The risk was higher in those with less reason to be suspicious of death by suicide based on prior difficulties!
A 2019 case-control study found a similar increased risk in Sweden:
The case group comprised 154 psychiatric patients (101 men, 53 women; age range: 13–96 years) who had committed suicide in Örebro County, Sweden. Control psychiatric patients matched by age, sex, and main psychiatric diagnosis were selected for each case. …
This study didn’t use “within subjects” control, which is a stronger statistical method, but found similar increased risk:
Benzodiazepine prescriptions were more common among cases than controls ( 42.2% versus 27.9%, p = 0.009, odds ratio: 1.89). This association remained significant in a model adjusted for previous suicide attempts and somatic hospitalizations (odds ratio: 1.83).2
In this cohort, no other medicines were associated with increased risk:
No statistically significant differences were seen between the groups in the use of any other subtype of psychopharmaceutical agent.
A 2017 review of 17 other trials all found, consistently increased suicide risk with benzodiazepine exposure:
Results: The majority of studies found that benzodiazepines were associated with increased suicide risk. This finding was consistent across various populations and different types of research, including a placebo-controlled crossover trial, a laboratory model of suicidal behavior, case-control studies regarding completed suicides on inpatient units, and large naturalistic studies.3
Caveat…Emptor
Essential caveats include those numbers only capturing individuals who were hospitalized for an attempted suicide, which biases the attempt numbers in the French sample downward:
In the before-times (Pre- COVID-19), a greater percentage of suicide attempt cases were admitted in the US from the ER vs Discharged. Still, we can conservatively add about 30% to the number of not-admitted suicide attempt cases to the numbers above, just by including cases presenting to the ER and leading to discharge:
In 2017, 64.4 percent of ED visits related to suicidal ideation or suicide attempt resulted in the patient's admission to the same hospital (30.1 percent) or transfer to another short-term hospital or another type of facility (34.3 percent). Only 34.6 percent of ED visits related to suicidal ideation or suicide attempt resulted in the patient being discharged home or to home health care (routine).4
The Arrow of Causation
With case-control studies, causation can not be proved. We also can’t ethically prescribe benzodiazepines at a massive scale to see if more of them will complete suicide. It would be akin to asking an IRB to approve a study (to quote my friend Nolan Ryan Williams, M.D.) “where we ask 100 people to wear motorcycle helmets and 100 people to take them off, and just run laps around Stanford’s campus.” That would be unethical.
We can not determine if the suicide risk is due to the benzo exposure or an unobserved common factor: maybe doctors are more likely to prescribe benzos to people whom they have a sixth sense about? Is the underlying risk for suicide psychic anxiety? It could be imagined to be a common factor driving both suicide and the additional Benzodiazepine prescribing.
However, what we can say is that benzodiazepine medicines don’t make the situation better, similar to the argument I have made about psychiatric hospitalization.
Zoom Out: It’s A Crisis.
As a child psychiatrist, in the broader context of worsening suicidality among both youth and everyone, the failure of benzodiazepines to make the situation better is notable, especially given the rates of prescribing in inpatient settings.5
As a child psychiatrist, I like to focus on vulnerable youth, and they are not being helped by the current system.
We already know hospitals in the US are being filled to the brim with children and others who have attempted suicide. Still, we also know not all suicide attempts result in medical or psychiatric hospitalization. According to the CDC, emergency department visits are also up among youth in the US.
During 2020, the proportion of mental health–related emergency department (ED) visits among adolescents aged 12–17 years increased 31% compared with that during 2019.
We don’t know how much, if at all, this trend has contributed to increased benzodiazepine prescribing and if that exposure leads to increased risk of suicide. We do know about a range of other risks that are beyond the scope of this article.
So what do we do about anxious people who might be dying more because of benzodiazepines?
I think there is a simple answer: better anxiety treatments that are not benzodiazepines and better treatments in the psychiatric emergency and acute care setting. We have hope on the horizon. Psychedelic medicines like LSD have promising early clinical data and more coming in GAD (pre-print from my group). We have FDA cleared neuromodulation for anxious depression. These treatments should move into acute care settings. SAINT fMRI guided accelerated neuromodulation in acute care settings needs broader deployment and payment models beyond Medicare.
We need to do better and avoid reliance on benzodiazepines which do not reduce risk, even as they alleviate symptoms in the here and now. We need to heal, not just salve a wound which festers, inevitably, for some.
The CCO analyses were performed in patients with an identified suicide attempt or suicide and with at least one dispensing of benzodiazepine in the preceding 120 days. Since benzodiazepine treatment is issued for a maximum of 30 days in France, we considered periods of 30 days for exposure assessment. The odds of benzodiazepine use were compared between the risk period (days −30 to −1 before the suicidal act) and two matched reference periods (days −120 to −91, and −90 to −61 before the suicidal act). Benzodiazepines dispensed on the day of the act were not considered. A washout gap of 30 days between risk and reference periods prevented any residual effect of an exposure in reference periods on the act.
Cato, V., Holländare, F., Nordenskjöld, A. et al. Association between benzodiazepines and suicide risk: a matched case-control study. BMC Psychiatry 19, 317 (2019). https://doi.org/10.1186/s12888-019-2312-3
Dodds TJ. Prescribed Benzodiazepines and Suicide Risk: A Review of the Literature. Prim Care Companion CNS Disord. 2017 Mar 2;19(2). doi: 10.4088/PCC.16r02037. PMID: 28257172.
https://hcup-us.ahrq.gov/reports/statbriefs/sb263-Suicide-ED-Visits-2008-2017.jsp
In contrast, 80.6 percent of all other ED visits resulted in routine discharges, whereas 14.3 percent were admitted to the same hospital and 2.8 percent were transferred
Johnson CF, Nassr OA, Harpur C, Kenicer D, Thom A, Akram G. Benzodiazepine and z-hypnotic prescribing from acute psychiatric inpatient discharge to long-term care in the community. Pharm Pract (Granada). 2018 Jul-Sep;16(3):1256. doi: 10.18549/PharmPract.2018.03.1256. Epub 2018 Sep 26. PMID: 30416628; PMCID: PMC6207358.
Blows me away how the new folks continue to repeat history. First we had the chronic pain cocktails of opioids, benzos, and amphetamine cocktails. The denial that addiction occurred when treating chronic non cancer pain (thanks pharma and highly paid MD shills!), and now I’m seeing buprenorphine and benzos combined for addictions that aren’t even opioid based with the idiocy of “meet them where they are.” I’m amazed at how duped prescribers get.
Your prolific writing continues to edify, explore, and open up issues for further discussion. Without knowing other meds used (or not) how can medical practioners extrapolate the association is benzo use? As a lay watcher of the post-Columbine luvox scare, seems an onset of SSRI / SNRI as “first line” anxiety tx also has created issues. Now, with the opioids crisis and the way benzos potentiate that class of pain meds, my region clinics REFUSE to prescribe the numb-out calmer downers. So the meth-psychotic turn to guess what? Opiate downers. I just -- question whether really we need Qualuudes to come back. (Only slightly joking.). Thanks for this column, Dr Muir. I fell in love w Frontier Psychiatrists on Clubhouse c. 2021.