

Mental Health Parity: What do Shaggy and Big Insurance Have in Common?
Mental Health Parity: What do Shaggy and Big Insurance Have in Common?
They have a similar strategy as it relates to compliance!

This is the second in a many-part series on mental health parity, the MPHAEA enforcement, and the Department of Labor’s new open comment period! Check out Regulations.gov, and feel free to leave an open comment on the proposed rules!
Honey came in and she caught me red-handed
Creeping with the girl next door
Picture this, we were both butt-naked
Banging on the bathroom floor
How could I forget that I had
Given her an extra key
All this time she was standing there
She never took her eyes off me
—Shaggy, “Say it Wasn’t Me”
However, DOL guidance can be hard to follow, so I’m using Hip Hop, R+B, and more to explain what the law means and what you can do. I’m Owen Muir, M.D.—a psychiatrist, dual board certified in child and general psychiatry. Please subscribe to support my work and share to support it more.
Shaggy wrote a great song about cheating, a problem with REPORTING REQUIREMENTS, and ENFORCEMENT STANDARDS. Cheating is the “NQTL” of relationships.
Healthcare organizations have problems with mental health parity. Today, we will address a specific issue, NETWORK SUFFICIENCY.
The law passed by Congress—the Mental Health Parity and Addiction Equality Act (MHPAEA), was designed to enforce access to mental health services. It did not work. Plans didn’t comply. They Cheated. This cheating has been denied. So the DOL is updating its guidance. Here is a secret transcript from insurance industry insiders:
Yo
(Open up, man) What do you want, man?
(My girl just caught me) You let her catch you?
(I don't know how I let this happen) With who?
(The girl next door, you know) Man
(I don't know what to do) Say it wasn't you
(Alright)
Sorry, that is Shaggy. My bad.
This update is not because plans were not cheating—it’s because they WERE CHEATING. And now, to catch them, we need standards. Standards that will demonstrate cheaters cheating. Shaggy, who wrote the adorable song about cheating and getting out of trouble, recommends a strategy.
DENY REALITY. To Wit:
But she caught me on the counter (It wasn't me)
Saw me bangin' on the sofa (It wasn't me)
I even had her in the shower (It wasn't me)
She even caught me on camera (It wasn't me)
She saw the marks on my shoulder (It wasn't me)
Heard the words that I told her (It wasn't me)
Heard the scream get louder (It wasn't me)
She stayed until it was over
The Department of Labor addresses this issue in their proposed update! The goal of mental health parity law is as follows:
[everyone1] who seek treatment for [Mental Health Care2] do not face greater barriers to accessing benefits for such conditions or disorders than they would face when seeking coverage for the treatment of a medical condition or surgical procedure.
And that hasn’t been happening. One of the reasons is “ghost networks.” Ghost Networks are exactly what they sound like… their “insurance network” has no actual people who will see you for your condition. They list many, many providers, but those providers won’t see you or, often, aren’t really in the network. The term they use for CHEATER is NQTL. Don’t bother trying to understand what the acronym means. It means cheater. I promise.
The network doesn’t pay enough to make it worth anyone’s while to be in. Providers won’t take your insurance because your insurance pays them less than their time is worth, and often not even then. I wrote a whole article about original research on this topic!

The Department of Labor calls bullsh*t on plans:
However, disproportionately high use of out-of-network MH/SUD providers by participants, beneficiaries, and enrollees, as compared to out-of-network M/S providers, is evidence that MH/SUD providers may be available in those geographic areas but joining provider networks is not sufficiently appealing to them.
That is a polite way of saying “payer" relationships with providers of mental health services are so actively hostile as be addressed like a hostage situation (as reported by the remarkable Clear Healthcare Costs):
Their stories of repeated requests to leave a contract, long phone hold times, no response to emails, and appeals to the New York State Department of Financial Services are full of sad detail. And their stories don’t begin to represent the problems of patients who will be struggling with insurance themselves – who is in network? What will the insurer pay? And how much time do I have to spend on hold to resolve this?
It is not being received well:
“Some of these clients are going to go to clinics, and some of them are planning to stay with me. If I continue to see these people, and I don’t bill their insurance, I can lose my license for that. That’s insurance fraud when you take money from somebody, right?”
The Department of Labor is aware this is happening. So their proposed rules say the following:
Departments believe that plans and issuers that impose NQTLs related to network composition should be required to collect and evaluate relevant data on the percentage of covered and submitted out-of-network claims for MH/SUD benefits as compared to M/S benefits. Specifically, if the proposed rules are finalized, the Departments are considering specifying the relevant data that plans and issuers would be required to collect and evaluate for NQTLs related to network composition which would include data on the out-of-network utilization
The DOL writing “believe that plans…impose NQTLs” is directly saying, “We know you are cheating. Because NQTLs are against the law.
The DOL believes plans are violating the law…
But she caught me on the counter (It wasn't me)
Saw me [violating our agreements] on the sofa (It wasn't me)
I even had her in the shower (It wasn't me)
She even caught me on camera (Nah, it wasn't me)
And so to CATCH THE PLANS ON CAMERA…in this context, means the following:
Often a plan's or issuer's published or printed provider network directory includes providers that are not actively furnishing services to participants, beneficiaries, and enrollees in the plan or coverage (i.e., "ghost networks").32
The DOL would like to collect information that illustrates if providers are actually in the network. Are the in-network providers submitting claims demonstrating they are active in the network? If not, it is cheating. They want confirmation.
She saw the marks on my shoulder (It wasn't me)
Heard the words that I told her (It wasn't me)
The law is about parity…ok, so that means data on medical services and mental health services. And they spell out which data they will be interested in:
providers including child psychiatrists and psychologists; other psychiatrists and psychologists; psychiatric nurse practitioners; master's level MH counselors, marriage and family therapists, independent clinical social workers, and advanced social workers; non-master's level MH counselors; board certified SUD addiction medicine physicians; and other non-physician SUD professionals;
Heard the scream get louder (It wasn't me)
She stayed until it was over
[Medical and Surgical] providers, including cardiologists; neurologists; orthopedists; pediatricians; other specialty physicians; physician primary care providers (other than pediatricians); non-physician primary care providers; and non-physician specialty providers.
Honey came in and she caught me red-handed
Creeping with the girl next door
Picture this, we were both [out of compliance]
Banging on the bathroom floor
So they are installing cameras to catch cheaters…and anticipating cheating in those camera feeds:
Departments are considering requiring plans and issuers to collect and evaluate relevant data on the percentage of in-network providers actively submitting claims from the six full calendar months that ended 90 days prior to the month in which the comparative analysis was conducted.3
So the plans are to have comparable numbers of in and out-of-network providers across mental and physical health.
They don’t. I promise you they don’t. They don’t like Shaggy’s friend was in the middle of having sex with his neighbor and denying the reality of that to his theoretically monogamous girl:
How could I forget that I had
Given her an extra key
All this time, she was standing there
She never took her eyes off me
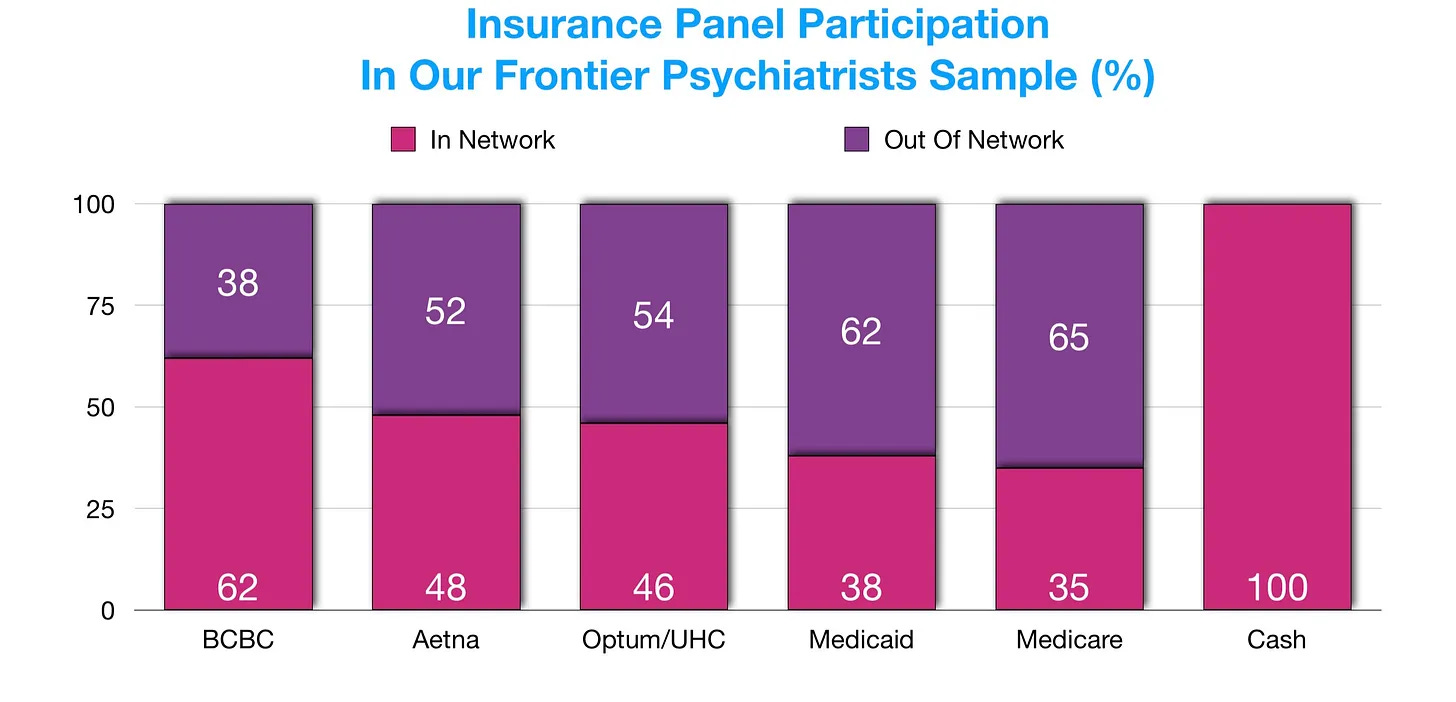
The response from payers can not be “oops.” Right now, our group’s original research suggests that mental health providers are not in the network at similar rates:
And in general medical care…for example, cardiology:
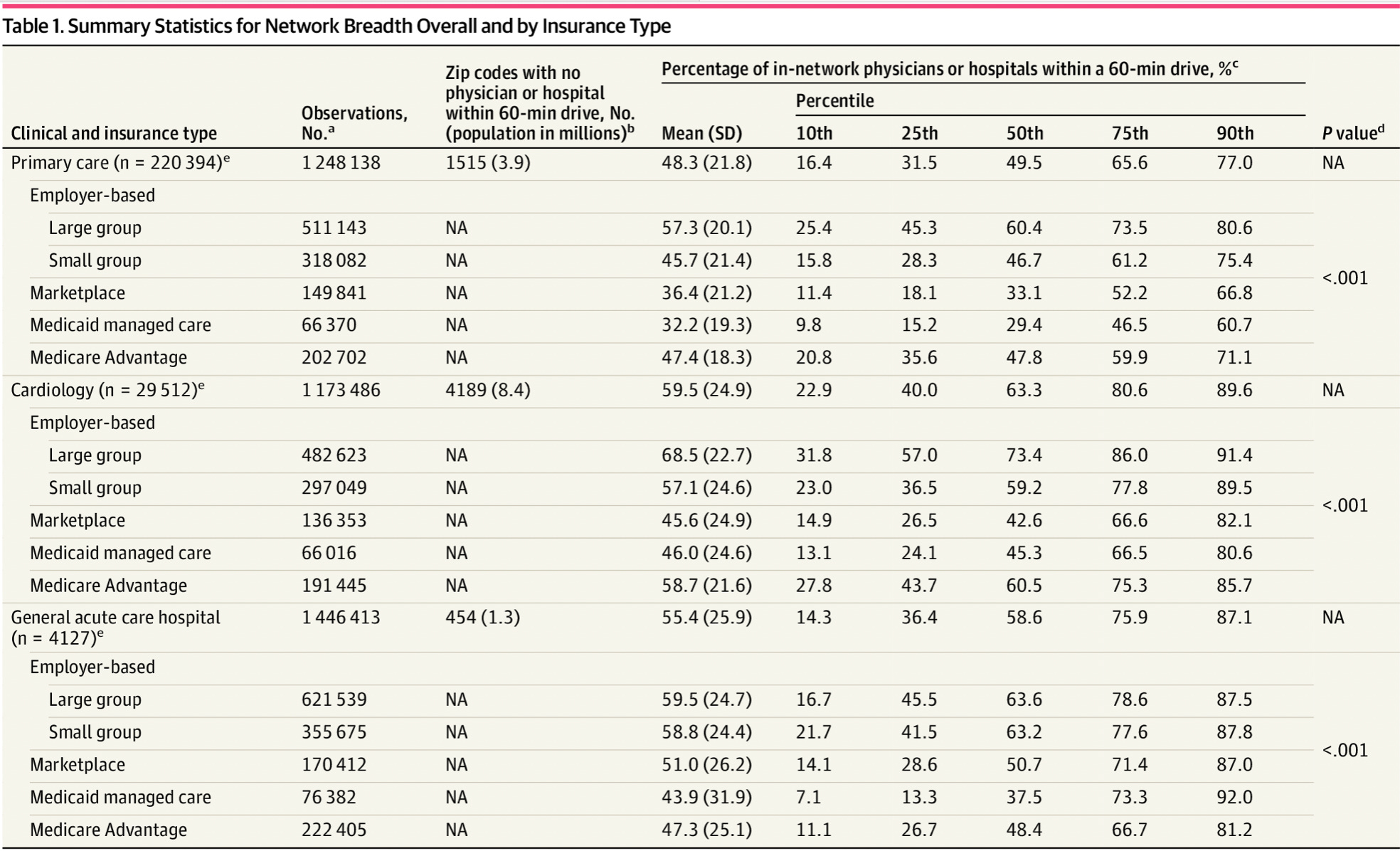
That is right. If there aren’t as many cardiologists and psychiatrists in the network…and therapists, and psychologists in the network, then the network isn’t compliant. That would be an NQTL. That would be CHEATING. The same for neurosurgeons. And interventional radiologists. The contracts for those individuals would need to support their decision to be in the network.
Right now, this is not the case…the following email came in just now while I was writing this…and Vikas Malik, M.D. from the Wonder Years clinic, agreed with me sharing it:
After multiple calls, we were able to get to a helpful rep who explained that they had a software update in April, which threw many providers out of network. We were advised to send a letter on our letterhead stating the providers that are in network with their NPI's along with a new W9 to Empire BCBS office on church street.
The turnaround time given to us was a pathetic 180 days.
This sort of thing becomes a problem if you legally need to have a sufficient network.
Remember that being a CHEATER in this context doesn’t mean a romantic breakup; your company becomes a TAX EVADER —not just for the insurance plan, but mostly for the employers purchasing the health benefits.
To make this painfully clear:
IF PAYERS HAVE NETWORKS THAT ARE NOT AT PARITY, the benefits they sell are no longer tax-exempt, legally. Parity is a compliance issue for EMPLOYERS, who have a fiduciary duty to MEMBERS. They NEED to have as many therapists, psychiatrists, and services in their network as they do all other kinds of care…it’s a crime. A jail crime. It’s not good enough to film-flam.
Gonna tell her that I'm sorry.
For the pain that I've caused
I've been listening to your reasonin'
It makes no sense at all
If we want to leave comments on this issue, the DOL requests we do so…
How can the Departments ensure that the data would provide a meaningful representation of whether a plan or issuer is [cheating]?
Can we catch ‘em on the bathroom floor?
Or this issue:
Should the Departments also require plans and issuers to collect and evaluate data on the total number of active in-network providers per participant, beneficiary, or enrollee to determine the percentage and the number of providers actively submitting claims?
My suggestion?
YES, PLEASE, GOD, MAKE THIS REQUIRED FOR REPORTING TO THE DOL.
Making mental health networks sufficient is only possible—if accurately measured—by paying mental health professionals MORE money for care that DRIVES DOWN utilization. The problem is too big to handle with scam ghost networks. We need access to the MOST effective treatments PAID MORE so that people will do them IN THE NETWORK. The therapist's time market rate needs to be the same as the network rate. If therapists and psychiatrists can make more money for less hassle doing work out of pocket and after taxes, that is a loss for patients, health plans, and health professionals.
We would love to be paid by insurance. It would have to be FAIR and, I don’t know, comparable to the rates across medicine. No more cheatin’!
That is what I have to say about NETWORK SUFFICIENCY. Please submit your comments supporting meaningful supervision of these requirements!
Please send comments via email to mhpaea.rfc.ebsa@dol.gov.
Honey came in, and she caught me red-handed
Creeping with the girl next door
Let’s ensure our relationship with our health plans is not the same as Shaggy’s relationship with the truth. His song—encouraging people to deny objective reality by “just saying it wasn’t you"— is intended to be FUNNY because it’s BAD ADVICE. It is not actual guidance for the behavior of humans. It is not appropriate behavior for massive companies. Call it out. Please share this article and submit comments accordingly. Part three is coming…
[Participants, beneficiaries, and enrollees in group health plans or group or individual health insurance coverage
covered MH (mental health) conditions or SUDs (Substance use disorder)
For example, for a comparative analysis conducted on February 1, 2026, the plan or issuer would be required to collect and evaluate data from May 1 – October 31, 2025.
Another insightful article and EXCELLENT use of Shaggy to help us laugh instead of cry at the spot on parallel.