


Fantastic Tissues and Where to Find Them: A Surgeon's Perspective on Endometriosis Tissues Across the Pelvis
Fantastic Tissues and Where to Find Them: A Surgeon's Perspective on Endometriosis Tissues Across the Pelvis
Like the beats found in the netherworld, endometriosis tissues take various shapes and forms. Today, we look at most frequently found.


Housekeeping: Today’s issue is media-heavy (has many images) so your email service may have clipped this message. If that has happened, don’t worry, you can expand the entire email using the link at the bottom or read this issue online in all its glory.
This week, we’re pulling straight out of J. K. Rowling’s reference stash and bringing to you a topic that has fascinated us and thousands of other surgeons across the world:
The expression of endometriosis across the pelvis.
Cells of an endometriosis tissue are similar to ones found in the endometrium, but they aren’t the same. They do react to the undulating hormones, but likely not in the same way as the endometrium does. This means they are, in popular internet meme speak, same same — but different.
They also react differently based on the vasculature present in the vicinity, and the nature of the underlying anatomy, giving rise to several different types (for the lack of a better word) of endometriotic tissue.
Today we go through 8 different types of endometriosis tissues, see how they appear differently in different places, and share some tips on how to dissect them. Our approach isn’t histological, but surgical. So we will focus on things that a surgeon needs to know, like the texture of a tissue, how to most effectively dissect it, and so on.
If any histologists are reading this, we would love to know your perspective in the comments below. So, let’s get started.
The first fantastic tissue type is the Red Riding Hood
Found largely across the peritoneum, in adhesions along the recto-vaginal plate and the pouch of Douglas, and often as endometriosis interna on the uterus; this type of tissue is heavily angiogenetic. Picking up on blood supply from around itself, this tissue bleeds upon touch and can sometimes even make a surgeon feel like they have ruptured a minor vessel.
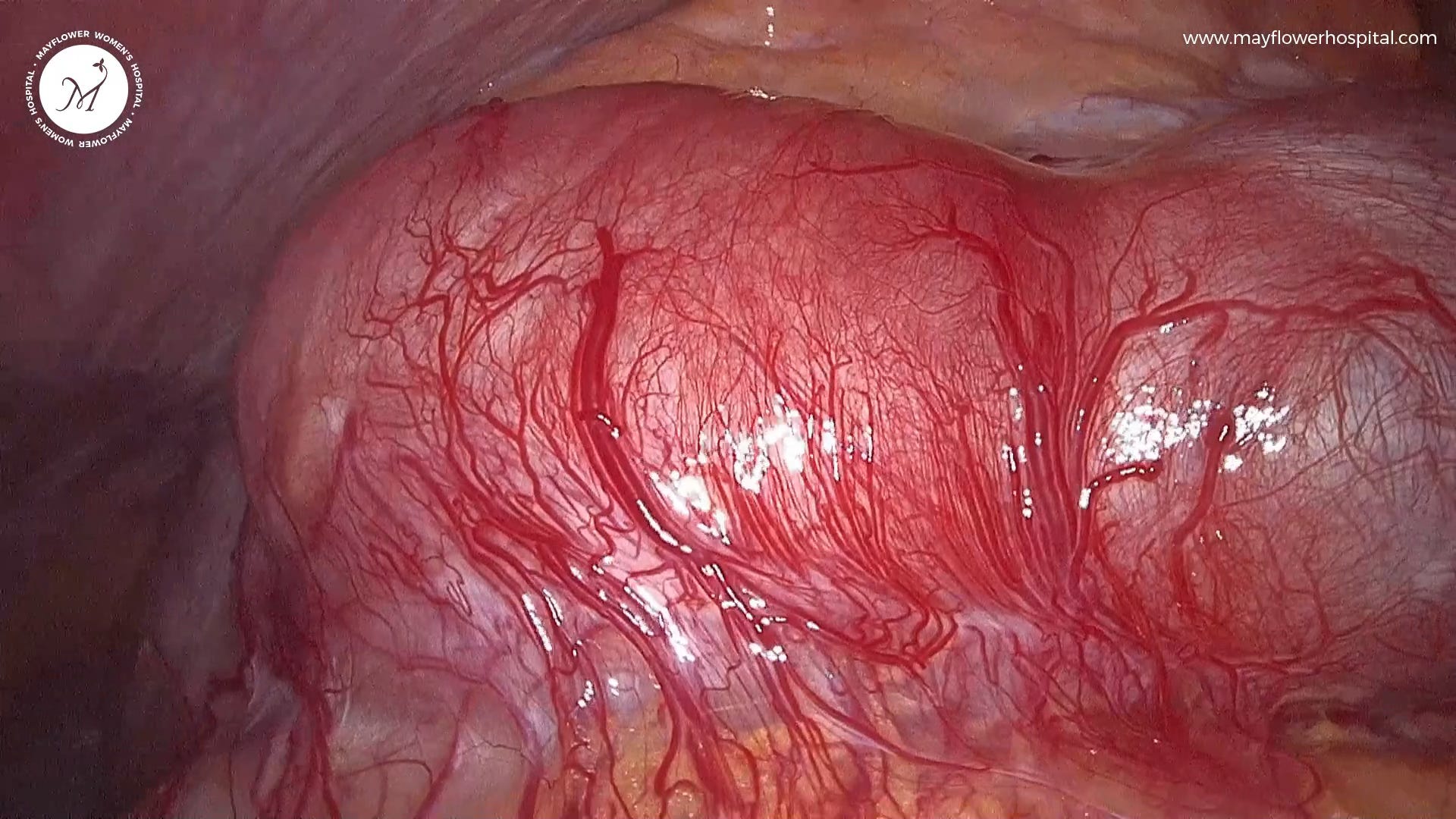
Mapping anatomical landmarks, and dissecting with proper coagulation when using an ultrasonic scalpel can help effectively handle this form of the disease.
The good news is that often the flush blood supply of the tissue gives a clear margin for dissection making the surgeon’s job a tad bit easier.
Next in Line are our fluid-filled cysts
The good old cysts of endometriosis, these tissues are found not only around the ovaries but almost all across the pelvis. One of the trickiest aspects of dealing with cysts is when they are several in number and staggered in position relative to your dissection plane. This always causes a problem as you keep encountering more cystic structures as you go deeper.
The key here is maintaining good traction and counter-traction to conduct fine and definite dissections. The best way to excise a cyst is to remove it en mass. Difficult as it may be, this approach saves us a lot of extra effort and cleanup that might be required in case of a cyst burst.
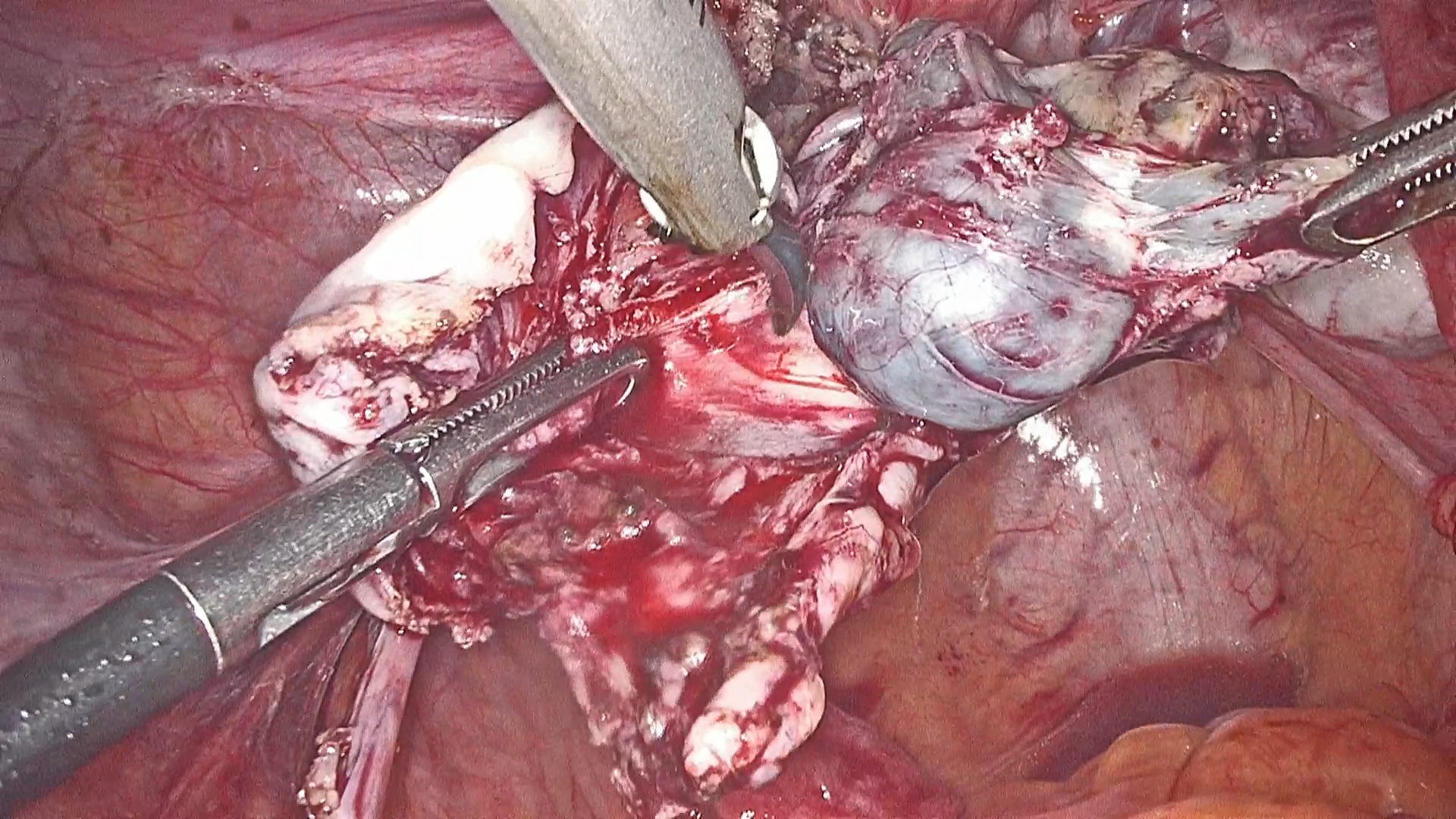
Moving on to Cystic Fibrotic Tissues
Probably the second most common tissue type in endometriosis, Plucky Peaches is a name this tissue gets owing to its fibrotic structure that encompasses cystic lesions within, almost like tearing a peach apart to discover its juicy interior.
Lying between the absolute fibrotic, and the complete cystic, these tissues typically present themselves in cases of adenomyosis and colonic involvement in DIE.
Like in the case of the heavily angiogenetic red riding hood, these peaches give away their appearance immediately upon dissection.
But whenever sighted they must be dissected completely. Leaving any trace behind might lead to rapid recurrence.
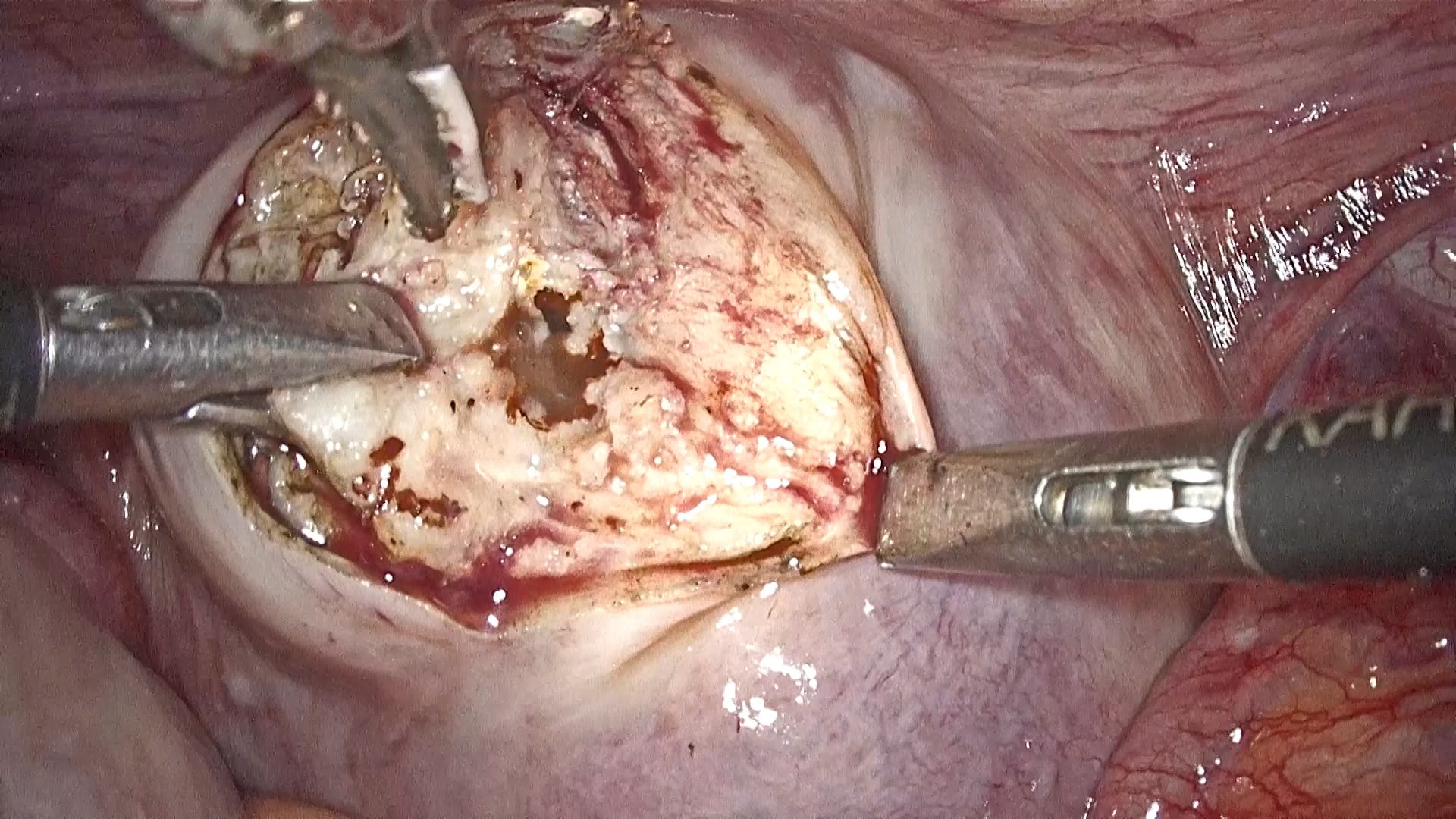
Next on our journey, we encounter a dense bundle of fibrotic tissues
Quite the opposite of an angiogenetic tissue, this fibrotic tissue type leaves very little room for vasculature or cystic formations inside of it. Some typical aspects of endometriosis like layer-by-layer growth, and an infiltrative nature are both well inherited in this tissue type.
However, dissecting this tissue only reveals similar-looking tissue underneath. On one hand, while continued traction and tissue stability are pros, one must be careful about the plane of dissection.
Owing to the fibrous nature of the tissue, it doesn’t necessarily give a definite plane of dissection, so it is advisable to derive its plane of dissection from the structures that surround it. Traction should be provided against the surrounding structures we wish to protect, and dissection should be done parallel to the endometriotic plaque.
The fibrotic, cystic, and angiogenetic tissues together form some of the base variants of endometriosis tissues. From here on, things start to get a bit complicated.
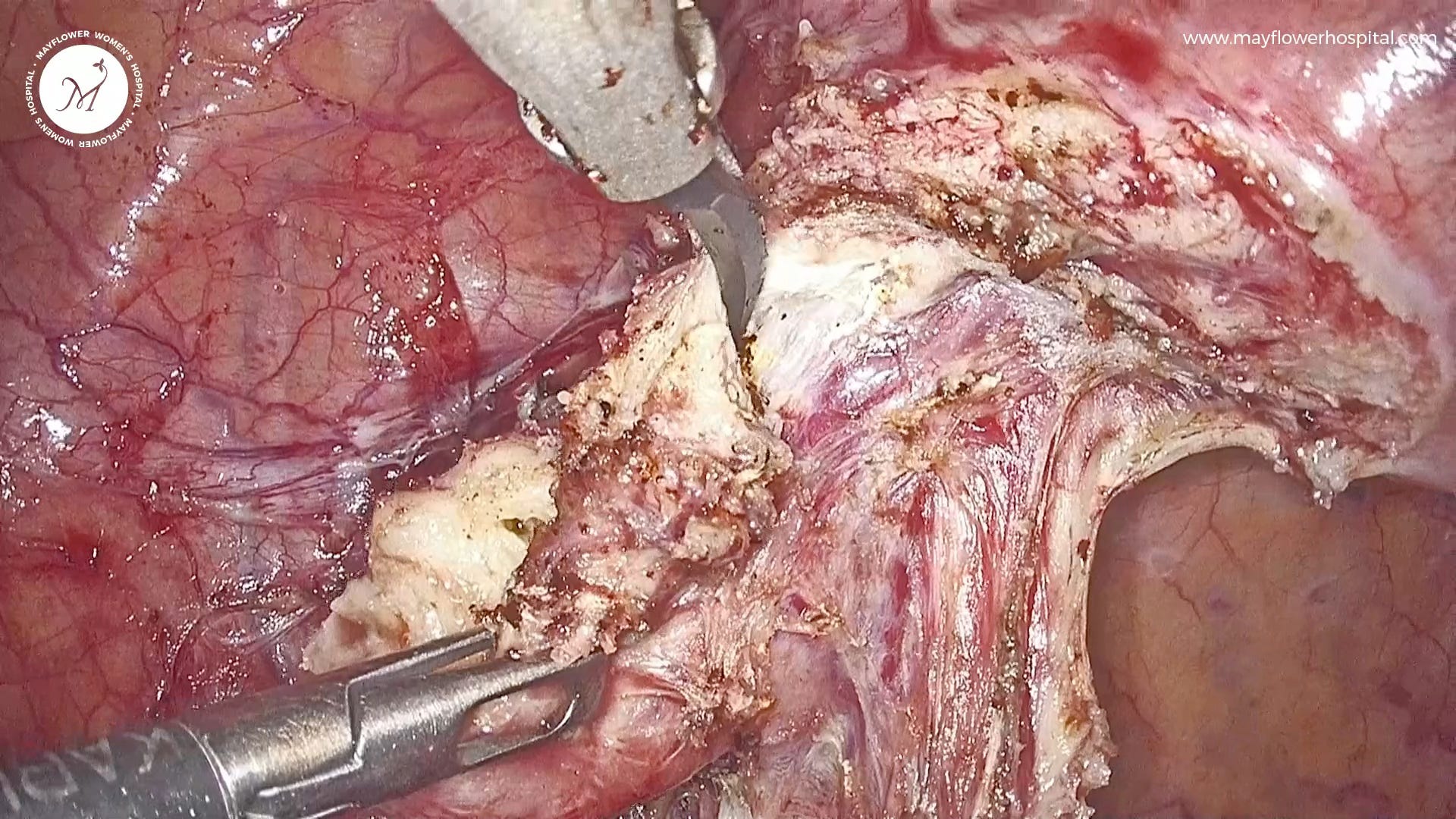
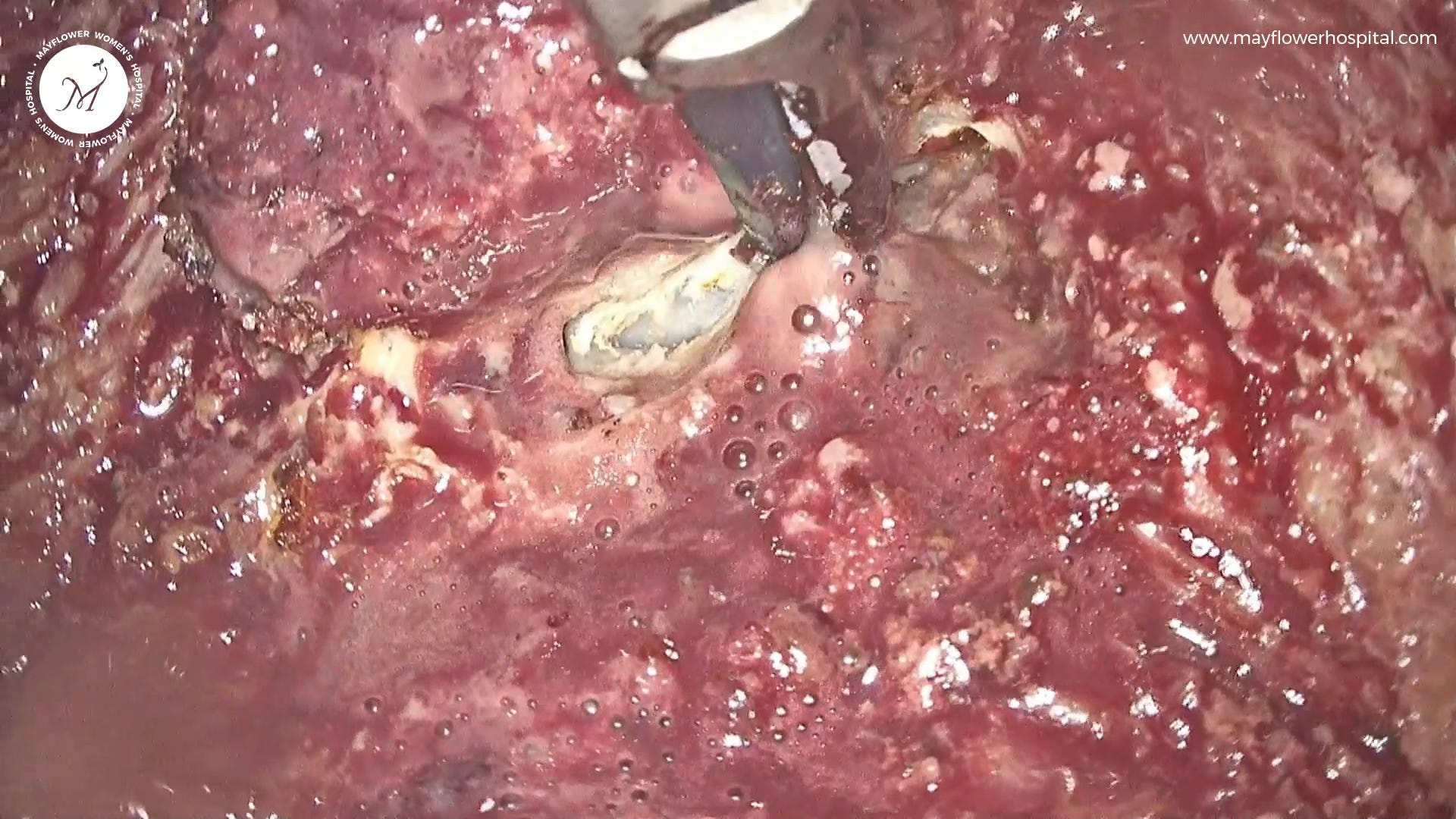
Our fifth tissue of the day is a drug-suppressed nodule
Born out of a suppression of growth following the long-term administration of GnRH agonists, these endometriosis tissues turn into thick, rubbery, dense masses with no clear planes of dissection.
Uncontrolled medical management of Endometriosis has several downsides and from a surgeon’s perspective, this is likely the worst. What’s seen below is the presentation of a nodule in a patient who had been administered GnRH agonists for 3+ years following an incomplete surgery for endometriosis.
You’re likely to get a better tissue response on the margins of the nodule where the organ is showing an inflammatory response. Dissecting as close to the margin as possible will ensure that tough, ungiving nodules are dissected easily and completely.
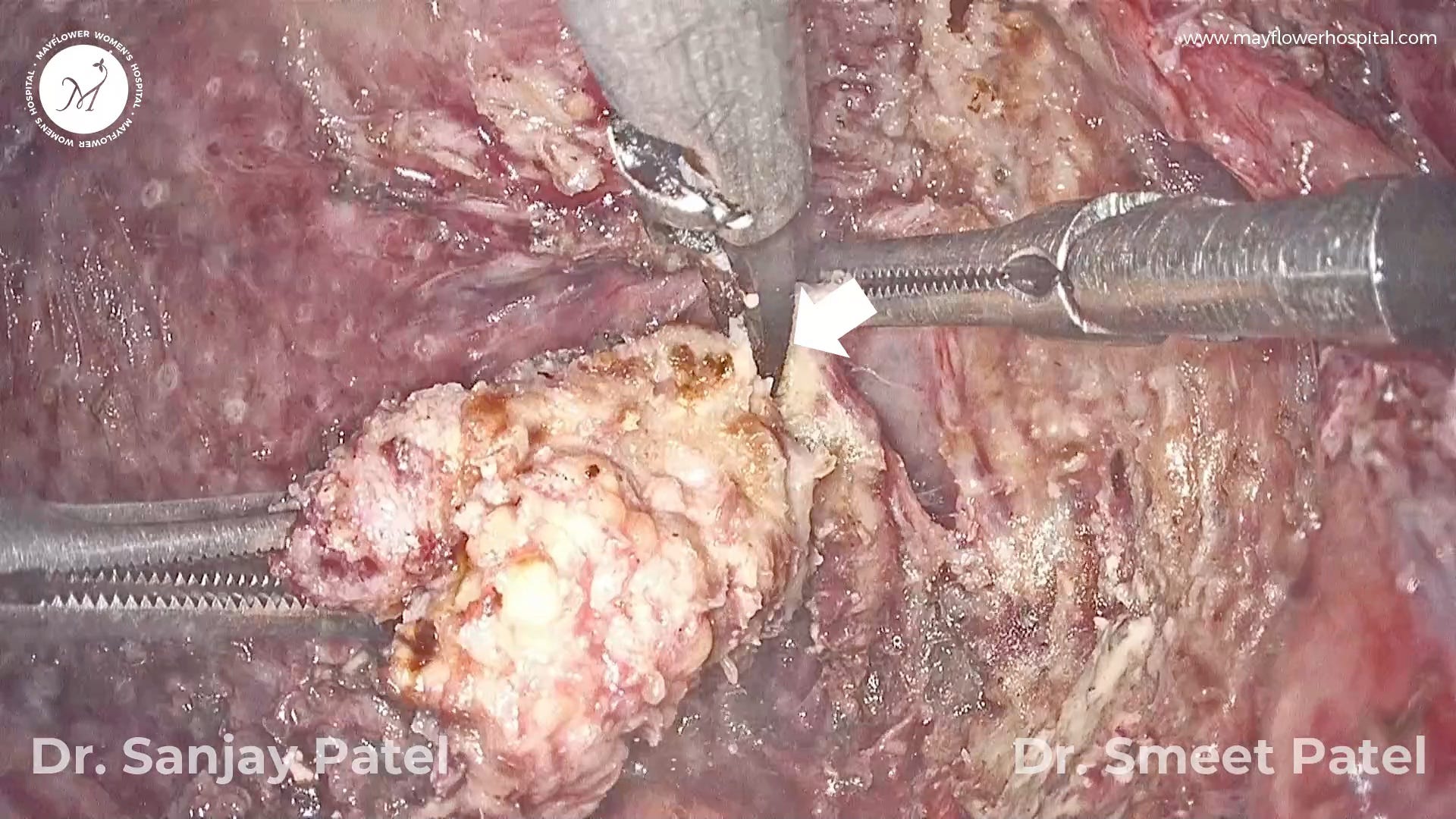
Tissue Six is an Active Glandular Tissue
The single tissue type to bear the most resemblance to the internal lining of the uterus is the active glandular tissue that we dubbed The Resurrected. With visible spurts of growth, this tissue shows clear signs of active glands at work.
When found (often) in the recto-vaginal junction, this tissue type presents a dissection challenge. Fat associated with the tissue belongs to the rectum while a non-discrete margin separates it from the uterus.
The first step of course is to dissect along the length of the rectum in a line that keeps the fat with the colon. You might still end up with some remaining tissue towards the fat which needs to subsequently be removed. On the other side, we stay flush with the uterus and the posterior cervix while dissecting, sometimes taking with us a small bite of healthy tissue. The collateral damage can later be sutured if required.
A rather aggressive approach for this tissue is needed owing to its active glandular nature. Its proximity to the vagina and the rectum also lends it to symptoms like dyspareunia (pain during sex), and dyschezia (pain while passing stool).
Next in line is the fantastical Post Surgical Tissue Growth
We’ve always stressed that a complete removal of endometriosis tissue is key to lowering the recurrence rate of the disease. However, when residual disease gets left behind in the pelvis it flares up again, often with intensity, invading several surrounding areas and growing further than its originally resected margins in the form of adhesions.
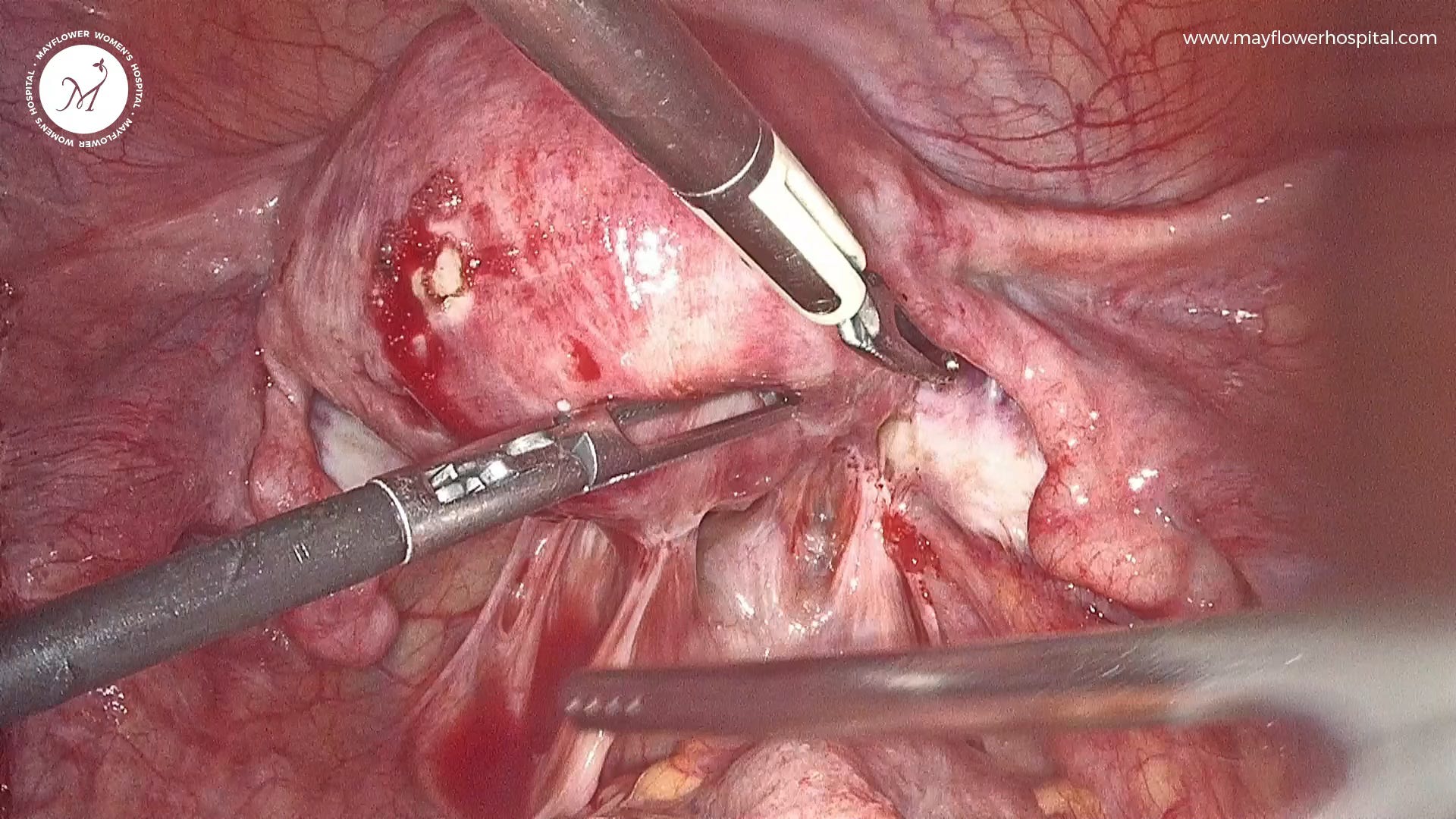
Endometriosis is a progressive disease and each tissue left behind in the pelvis is a seed for the disease to regrow later. This is why a total elimination of the disease and a complete restoration of the anatomy should be the goal of every surgery.
And the last tissue in our bunch is the Infective tissue
While an infective tissue isn’t a type in itself, it presents a whole new set of challenges and therefore deserves to be looked at separately from a surgical perspective.

Most dangerous when occurring on a cystic tissue, or an angiogenetic tissue, this particular type is often caused by a varying set of instances within the pelvis. An ovum pick-up procedure conducted in altered anatomy can lead to a needle piercing through the colon and into the ovary, leading to infection transfer. But this is just one example of a range of reasons that can make the pelvis infected. It may even be caused by a simultaneous occurrence of PID (Pelvic Inflammatory Disease) and Endometriosis.
The subsequent growth of endometriosis tissue may also propagate the infection worsening the trouble at hand.
Infected tissues require a thorough inspection of the type and intensity of infection, their involvement in surrounding organs, and the damage that they’ve already done. Your surgical decisions must therefore be made with wisdom.
That’s it!
That brings us to the end of the 8 Fantastic Tissues of Endometriosis that we saw today. And there could be many more. It’s fascinating to also note that any of these tissues can exist in conjunction with one another. An angiogenetic tissue can become infective, a fibrotic tissue left undermanned during surgery can flare up, and an active glandular tissue may give way to a cystic collection.
The world of endometriosis is far, wide, and incredible. And we hope to keep exploring it. Let us know what you think of this issue in the comments below. We love reading all your comments!
 | A guest post by
|
 | A guest post by
|
Nfpeterse@gmail.com